
Before you read this post/chapter of TruthsAboutHealthCare, you should read the post/chapter pasted below:
https://www.truthsabouthealthcare.com/wp-admin/post.php?post=64&action=edit
An excerpt a propo to this post/Chapter is this:
“On May 16, 2017, this article was published in JAMA (“Reassessing the Data on Whether a Physician Shortage Exists”; JAMA May 16, 2017, Volume 317, Number 19). Here is an excerpt:
“The United States currently has more than 900,000 active physicians. Of these, 441 735 are primary care physicians and 484,384 are specialists. Approximately 12% of primary care physicians work part time, leaving slightly more than 388,000 full-time primary care physicians. Of these, nearly 80 000 are pediatricians. According to recommendations from the Agency for Healthcare Research and Quality, the average physician panel size—the number of unique patients under the care of an individual physician—should be between 1500 and 2000. A recent Medical Group Management Association survey of primary care physicians found that the median panel size was 1906 and the average was 2184. Conservatively, if each of the 388,000 full-time primary care physicians cares for an average of 1500 patients, they could care for an estimated 583 million people. Today, there are 240 million adults in the United States. Even at the low panel size of 1500 patients, all adults could be cared for by 160,000 primary care physicians; at a panel size of 2000 patients, the United States would require an estimated 120,000 full time primary care physicians. Similarly, the 73 million US children younger than 18 years could be cared for by an estimated 49,000 pediatricians, assuming that each provides care for 1500patients, or by an estimated 36,500 pediatricians with panel sizes of 2000 patients. Add to these conservative calculations the care provided by the more than 50,000 part-time primary care physicians and there seems a significant surplus, rather than a shortage, of full-time primary care physicians.”
The thing is, you can find many articles and projections and you hear on the news all the time that the US needs more doctors and advanced practice clinicians (APC) (combined to be referred to as “Providers”).
I’m going to expand on why this dichotomy in thinking exists. The main reason being that the supporters of more Providers is they completely lack knowledge into what are the drivers of their conclusion that are not going to be solved by just adding more Providers.
Let’s just take Primary Care Providers (PCPs). Why can’t the current number of PCPs take care of 320,000,000 US people?
Problem #1: Inefficiency of the US health care system.
The US health care system is incredibly wasteful, as described in the post attached to this URL:
https://www.truthsabouthealthcare.com/wp-admin/post.php?post=280&action=edit
It’s been well established by efficiency gurus like Joseph Juran that the more inefficient a system or process is, the more people you need to run the system or process to offset the inefficiency. To illustrate this point, here is a fictitious analogy.
A burger joint opens. It is the only burger joint for 50 miles. The burgers are good and cost 50 cents each. The critical step in the delivery of burgers to the customer is “grill the burger”. The burger joint has one griddle in the joint and it can only grill four burgers at a time. When the burger joint first opens, there are few customers, everything goes well, people get their burgers in 2-3 minutes. Soon, the word is out that the burgers are really good, and more customers arrive. Due to the limited number of burgers a griddle employee can cook at one time, the wait time for a burger increases to 10-15 minutes. People start to complain. To assuage the customers, the burger joint owner tells the customers every 2 minutes that they will be getting their burger soon, assuming as long as people know they will eventually get their burger, customers will complain less.
The burger joint owner then installs another four-patty burger grill and hires another griddle staffer to man the griddle. Because of the cost of the griddle and the new employee, the burger joint owner has to increase the price of the burger by 20%. People grumble but anti up the new price as the wait time goes down to 5 minutes. Again, more and more customers frequent the joint and the wait time increases. The burger joint owner installs two more four-patty griddles and hires two more griddle staffers. The price goes up to $0.90, but the wait time is back down to 5 minutes. Customers are angry about the price increase but, they can’t drive 50 miles to another burger joint and so they simply pay the price.
This is how the US health care system works today. Add more people into an inefficient system, replicate that inefficient system in new clinics and hospitals and just up the price because health care is what, in economics, is called an “inelastic product/good”. In economics, this means you can increase the price and the demand will stay relatively the same because people really need it. Gasoline is a similar inelastic product/good. Health care administrators know this fact, so, rather than trying to fix the system, it is more lucrative to build more revenue centers and install the same inefficient processes. Besides, they can just continue their cost plus strategies. People will pay anyway. And besides, the people don’t know that there is a better way to do things. Easy decision for the bean counters.
The real solution to the burger joint wait time problem is to rip out the four-patty grill and install a 16-patty griddle manned by one staffer. The price increase would have been only a nickel and the wait time would have stayed at 2-3 minutes.
The inefficiencies in the health care system are incredibly numerous. There are six chapters about this at truthsabouthealthcare.com. Here’s a short list at the PCP level:
- Low performing clinic throughput systems (registration, rooming patients, the EMR, etc.)
- Provider-centric patient scheduling. For example, all appointments are in 30-minute intervals, all new patients (no matter the patient complaint) are scheduled for a 40-60 minute appointment, start and stop times inconvenient for patients, etc.)
- Days and times Providers are available are Provider centric and not in synch with peak demand times or patient preferred times and days.
- Time spent on inquiry that duplicates or triplicates already documented facts that are readily available.
- Rooms, like Treatment Rooms, that lie vacant >90% of the time, when they could be used as exam rooms.
- Exam rooms “saved” for patients who are undergoing testing, reducing the availability to move patients through the clinic. (in other words, a patient has a test ordered where they have to vacate the exam room they were in and the exam room remains empty while they are getting the test, instead of rooming a new patient in the exam room and having the patient consult with the Provider about the test in the Provider’s office.)
- Not utilizing Nursing staff to do tasks within the scope of their licensure, having Providers do those instead. Things like reviewing test results and notifying the patients with normal results or abnormal results after consulting the Provider about the care plan.
- Not having pre-set-up “kits” for things like laceration repair or pelvic exams so staff don’t have to search and collate the necessary materials.
- Not having exam rooms set up to provide Providers with what they need with minimal movement. Like, instead of tongue depressors being in a drawer or jar, have a dispenser on the wall next to the oto/ophthalmoscope so that a Provider can reach one without moving from the exam table.
- Providers refuse to do add-on appointments for their own patients, creating a daily fixed number of patients they will see. This is why Walk-in and “minute-clinics” are doing so well.
I’m sure there are more, but I think you’re getting the point.
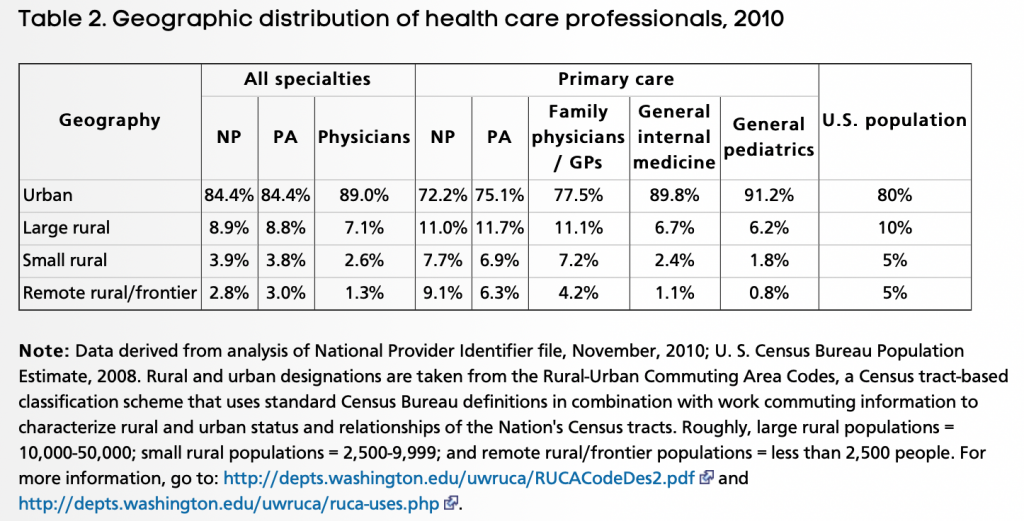
Problem #2: Distribution of PCPs.
While not as extreme as some would have you think, there is somewhat of a preference for PCPs to practice in urban areas. See figure below from AHRQ. (Reference: https://www.ahrq.gov/research/findings/factsheets/primary/pcwork3/index.html)
At the same time there is a significant issue with distribution among states and among counties within states, especially the larger more rural states. Patient to PCP ratios, for example in a state, can range from 700:1 to 3000:1. There is obviously a PCP supply problem in the county with a 3000:1 ratio. For example, go to this URL to see the distribution by county for New Mexico: http://www.countyhealthrankings.org/app/new-mexico/2018/measure/factors/4/data
Problem #3: More Providers are part-time.
More than any other time in US history, physicians and APCs are working part time, and their colleagues decline seeing their patients when they are not in the clinics. Patients have to wait. For acute problems they go to Urgent Care. Their skewed access metrics contribute to the idea of Provider shortages.
Problem #4: Failure to successfully implement a team model that optimizes the skills, licensure and availability of each team member. There are pockets of these models, but only a few function well, and often the team members are stuck in the same set of issues outlined above in the inefficiency section.
Problem #5: Inability to “mass customize”.
Health care systems, including PCP offices, try to put all patients in the same “box”. The same time slots, the same rooming procedures, etc. no matter what the patient type or their problem or problems. It’s like everyone having to have the same smartphone with the same apps on it, or the same computer with the same RAM and disk space and features.
I’m sure this isn’t all of it, but you see what I mean. Instead of improving the systems that Providers and patients are stuck in, people will advocate for more Providers. We can’t sustain the increase in brick and mortar and people (like the burger joint griddles and staff). It’s time for a major shift in thinking and action.
Oops, I forgot, the people running the health care systems are incapable of mustering up that shift. Same ol’ same ol’ persists. The sacred cows are still munching. The leaders are clueless.