
Why It Is so Difficult for Health Care Systems to Perform to Expectations
Health care institutions and systems have existed in the US since colonial times. Globally, even longer especially in Europe. You would think that by now, running health care systems would be so refined and reliable that they would beat out the airline and nuclear energy industries.
Regrettably, this is not true. A recent British Medical Journal article cited Medical Errors in the US accounted for ~250,000 deaths and was the third highest cause of death in the US (Medical error—the third leading cause of death in the US.; Makary MA, Daniel M. BMJ. 2016;353:i2139.) This number is larger than the numbers previously reported by the Institute of Medicine because the IOM numbers are inpatient cases only. Mr. Makary, through the use of other information sources, “extrapolated” the data to estimate the rate for the US population, which would include ambulatory deaths.
That would give one pause. But the situation is even broader than this. US health care systems are notoriously inefficient. They are highly reliant on people providing their products. And generally people have a 2 sigma error rate (95% accuracy) when they are doing only one thing at a time. This can fall to 1 sigma (68%) if they are doing more than one thing at a time, especially complex tasks, which are common in health care. There is abundant waste in health care, estimates by the Rand Corporation and the Institute of Medicine being in the range of 30-40% waste. No other industry/business would accept this level of waste. Definition of waste: an act or instance of using or expending something carelessly, extravagantly, or to no purpose.
The US health care system is guilty of all three of the “acts” in the definition.
So, why is this? Why is it that health care systems, which have your LIFE at stake, are so inefficient, wasteful and error prone?
Here are the reasons.
- The administrators that run the health care systems are mediocre.
- There is a lack of physician leadership.
- Most clinical managers in health care are licensed clinicians who never had any formal management training.
- Health care management training is woefully inadequate.
- Health care management is a task oriented management system vs. a process management system.
- The answer to any business/operations problem in health care is: add more people
First, let’s go over some definitions.
What is the definition of a “leader”? Depends on whom you ask!
The MBA-types would probably articulate something close to this definition from the Business Dictionary (businessdictionary.com) – A person or thing that holds a dominant or superior position within its field, and is able to exercise a high degree of control or influence over others. (This definition almost sounds fascist.)
Merriam-Webster definition – a person who leads. (Pretty vague.)
Dictionary.com definition – a guiding or directing head, as of an army, movement, or political group.
Gallup definition from “The One Thing You Need To Know” – Leaders provide a vision and are able to motivate people to follow them to achieve that vision.
Team Technology definition – Leadership is setting a new direction or vision for a group that they follow, ie: a leader is the spearhead for that new direction.
In my experience, the Gallup and Team Technology definitions are more closely related to superior performances.
What’s the definition of a “manager”?
Business Dictionary – An individual who is in charge of a certain group of tasks, or a certain subset of a company. (More concrete than leader)
Merriam-Webster – a person who conducts business or household affairs.
Dictionary.com – a person who has control or direction of an institution, business, etc., or of a part, division, or phase of it.
Team Technology – A Manager controls or directs people/resources in a group according to principles or values that have been established.
Go2HR.com:
“The main difference between leaders and managers is that leaders have people follow them while managers have people who work for them. A successful business owner needs to be both a strong leader and manager to get their team on board to follow them towards their vision of success.”
The difference between a leader and a manager is important. Not all people in positions of leadership can actually really lead. They act more as managers than true leaders. This is the biggest issue in health care. Who people call (or call themselves) leaders are actually just managing. This creates inertia, because there is a lack of vision.
The administrators who run the health care systems are mediocre.
I’m here to tell you, it starts at the top. And by the top, I mean the C-suites in health care. The administrators. The MBA’s who are supposed to be running the operations of the health care institutions in our country. Essentially, there is a lack of effective administrative and physician leadership in health care. Let’s start with the administrators.
The “MBA-types” running the health care systems and institutions in the US are generally “C-players”. Oh, there’s an occasional B minus- player, and they stand out and appear to be A-players, but, really, they are B minus-players in a sea of C or less players. I have personally never seen such a group of rigid thinking, uncreative, and just plain underachieving people when it comes to administrators running health care systems. Their forte’s are building buildings, starting up new services, like a day surgery center, and manipulating finance numbers to maximize profits. For the rest of running a health care system, they are woefully inadequate.
The main reason for this is, the A and B-players are in industries that require brains and assertiveness and pay a heck of a lot more for it. Unless an MBA is in the upper echelons of a multiregional or national health insurance company, they don’t get paid nearly as well as, say, a Donald Trump business executive, someone on Wall Street, someone at GE, someone at Bank of America, etc. So, the health care industry attracts the next levels down. The ones that can’t make it in the higher-powered industries. The below B-players. The smaller the hospital, the lower the GPA score. Yes, all the way down to the “F” level.
I can’t tell you how many times I’ve sat across a health care administrator’s desk, explaining something four different ways and they sit there looking like a deer looking into headlights. The sad part was, they and their MBA colleagues discount what the clinicians say or propose. Mainly because they don’t understand it. And clinicians are generally smarter than the health care level MBA-types. That’s why they hardly ever get along, the clinicians can see through them. The MBA’s don’t like that.
Now, I’m not saying there aren’t any C or less clinicians, there certainly are! But they don’t control complex services impacting thousands and thousands of patients.
I already told you about the COO who stated we didn’t have to do anything urgently about patient safety because it had been going on for a long time. And the administrator who thought it was unnecessary to train ICU nurses.
Here’s another true story about how these MBA guys operate.
I started a job as the Regional Medical Director of a Staff Model HMO. The Regional Administrator and Regional Marketing Manager were vacant positions. There was a part time HR manager. That’s it, me and a part time HR manager.
Since I had done some contracting with provider offices in another position, I was tasked with contracting with the HMO’s network providers. This was usually part of the administrator’s job. I had never contracted with a hospital before, but I understood their operations. The Contracting Specialist had initially been hired to be the Regional Administrator but was demoted (hence the vacant Regional Administrator position. See what I mean about C-players?). So, the MBA was incapable of doing this work and they tasked me, the DOCTOR, to do it.
The Contracting Specialist for the region and myself sat down with the executives of the first hospital on our list. My strategy was to try to understand their cost structure and then fashion a deal where we both “made out”. I had studied books like “Getting to Yes.” I started the conversation by saying we didn’t want to ratchet down on the hospital fees we would pay to the detriment of the hospital but I also couldn’t afford them a lucrative fee schedule that would negatively affect our health plan budget for health care services.
Now, hospital contracts have two general “sections”: Inpatient and Outpatient. Inpatient was pretty simple in those days, a DRG (lump sum per admission) or a Per Diem (lump sum per day). It was the Outpatient that was complicated because of the multiplicity of services (Lab, X-ray, PT, ER, etc.)
My first category for negotiation was for Lab services. I asked the Execs if they knew the profit margins on the tests in their Lab, like, what was their margin on a Complete Blood Count (CBC). I used to deal with this in my private office, so I knew how this should go. In my practice, I paid a reference lab $10 for a CBC and charged $20 for it, so my margin was $10 or 100%.
The CFO and CEO said they didn’t have that data. I asked them if they knew if their Lab made money for them or lost money. They said they didn’t know. I shifted to the X-ray department and asked the same two similar questions: Did they know the margin for the X-ray tests or whether the X-ray department made or lost money. They said they didn’t know.
I asked them how they managed the financials of the hospital if they didn’t know where in the hospital they were making or losing money. They said they just looked at the total expenditures for the entire hospital then looked at their total revenue stream. If it looked like they weren’t going to meet their financial/margin goal they renegotiated insurance contracts for more money.
Is anyone reading this running a business? Is this how you operate? And remember, I’m the Doctor! There’s no MBA or HCA or any other business school acronym after my name!
They couldn’t target any areas where they were losing money and attempt to stop the hemorrhage. They just did what hospitals are wont to do – it’s called “cost plus”. You just look at the roll up of your expenses and manipulate the price to make a profit margin. This is the main tactic these MBA guys use and is a foundational reason why hospitals and health care systems are so inefficient. Instead of fixing where inefficiencies exist, they just price to pay for the waste.
Here’s another.
I fulfilled my obligation in the National Health Service Corp (NHSC) in 1985. During that NHSC tenure, I was a whistleblower on an administrator who was embezzling money from a “community” owned mini health care system. I had gained access to the financials and figured out what was going on. So, I got somewhat proficient reading financial spreadsheets. Part of the operation’s revenue was a capitated HMO contract. I got to see how this affected the revenue of the health care system, with all of the nuances of a capitated environment, like risk pools, withholds, etc.
In 1986, I was in a different state in a medical group with a significant number of patients as members in a capitated health plan contract. I was in a small satellite clinic, and the office manager would share the financial information with me. The way the plan worked was, we were given a lump sum per patient per month and we had to pay everything except hospital bills. I actually had one woman in a back office who paid the claims, was the Provider Services representative, and the Member Services representative. I did all of the Utilization review and non-hospital provider contracting. Yes, just two of us! Because of this situation, I was able to get a hold of the HMO contract.
After reading the contract, I met with the administrator of the medical group. I told him, my estimation was, the HMO contract was not a beneficial contract for the medical group. There was too much risk for the way the member premiums were being allocated between the HMO and the medical group, i.e., the group was being underpaid. He scoffed at me and told me the contract was a huge boon to the group. I complained to the physician leaders of the group (remember, I was the newbie) who told me the administrator knew what he was talking about, I should stop complaining.
Six months later, the medical group was on the brink of bankruptcy. Another HMO bought out the HMO with whom we had the contract. The new HMO’s initial assessment was, our medical group and three others in their merger and acquisition were on the brink of bankruptcy DUE TO THE ORIGINAL HMO”S CONTRACT!!!
Our medical group actually did go bankrupt. The other three survived because the new HMO revised their contract terms TO PAY THEM MORE FOR WHAT THEY WERE RESPONSIBLE FOR! Our group was too far gone by the time that offer arrived. Thanks to the administrator.
Here’s one more. I have about a hundred, but, you should be getting the point.
I’m in a four-physician clinic that belongs to a large multispecialty group. It’s been losing $500-750,000 a year. It’s only a three-year old clinic. I’ve been there a year and have been at the meetings where everyone is bemoaning the losses. The clinic consists of two Internists and two Pediatricians who are on call every other day and every other weekend. The office hours are 8:00 AM to 8:00 PM Monday -Friday, which means the physicians have to work in shifts: 8:00 AM-4:00 PM and 12:00 noon to 8:00 PM. There are Saturday morning office hours from 8:00 AM-1:00 PM. Whoever is not on call for the weekend staffs the Saturday clinic.
The clinic staff consists of two receptionists (one for the Internists and one for the Pediatricians), 1.5 FTE clerical, 1 FTE X-rays, 1 FTE lab tech and an office manager. There is a nurse for each physician.
The office manager quit. The medical group lead physician came to me and asked me if I will become the Medical Director of the site. I would be responsible for all of the operations and clinical areas. I had to hire another office manager. My main goal besides making sure the clinic ran well was to reduce the financial losses, for which the medical group administration couldn’t heretofore come up with a solution. (The MBA guys)
The first thing I did was start doing busy studies of everything in the clinic, compiling graphs of the frequency of use of services. I figured, if it was a good method for tracking vital signs, it should work for something like this. I had a graph for physician visits by day, session, hour, etc. I had graphs for number of X-rays per session, number of lab tests per session, number of cancellations, number of no shows, appointment slot vacancy rate, etc. No one had tracked these before.
What I found out were things like this:
In the evenings, the X-ray rate was 0-1 X-ray per session (mostly zero). The lab test rate was 1-3 per session (mostly 1-2). The no show, cancellation and vacant appointment slot rate was highest on Tuesday, Thursday and Friday evenings. We lost tons of money on those evenings between staff costs and wasted supplies (supplies in the lab and X-ray departments which had to keep things running despite not doing anything). The Saturday clinic was breakeven for Internists and the Pediatricians made money.
I suggested that the clinic close for the evenings on Tuesdays, Thursdays and Fridays and that there be no X-ray after 5:00 PM on days the clinic was open until 8:00 PM. This was initially met with resistance because the administrator kept saying we were closing at times when there was activity (revenue) opportunity. I finally convinced the physician leaders to try it for six months (they owned the medical practice).
In six months, we were running at breakeven. I guess they don’t teach operations measurement and improvement in those MBA schools.
There is a lack of physician leadership.
This is a national problem. Doctors are generally not admitted to medical schools for their leadership abilities. It is more for their academic achievements and their individual drive. They get no leadership or management training. They are trained to assess, diagnose and then give orders within a task oriented environment.
In my experience, only about 2% of the physicians in the US physician population are true leaders. Some of the other 98% get into leadership positions, but they are far from being leaders. And half of that 2% don’t want to leave their practices for leadership positions.
The thing is, when these true leader physicians get into leadership positions, magic happens. They can be truly transformative. Unfortunately it’s not a common occurrence.
Not that the non-true-leader physicians don’t assume leadership positions. Here’s a figure from the 2017 Medscape Physician Survey about it.
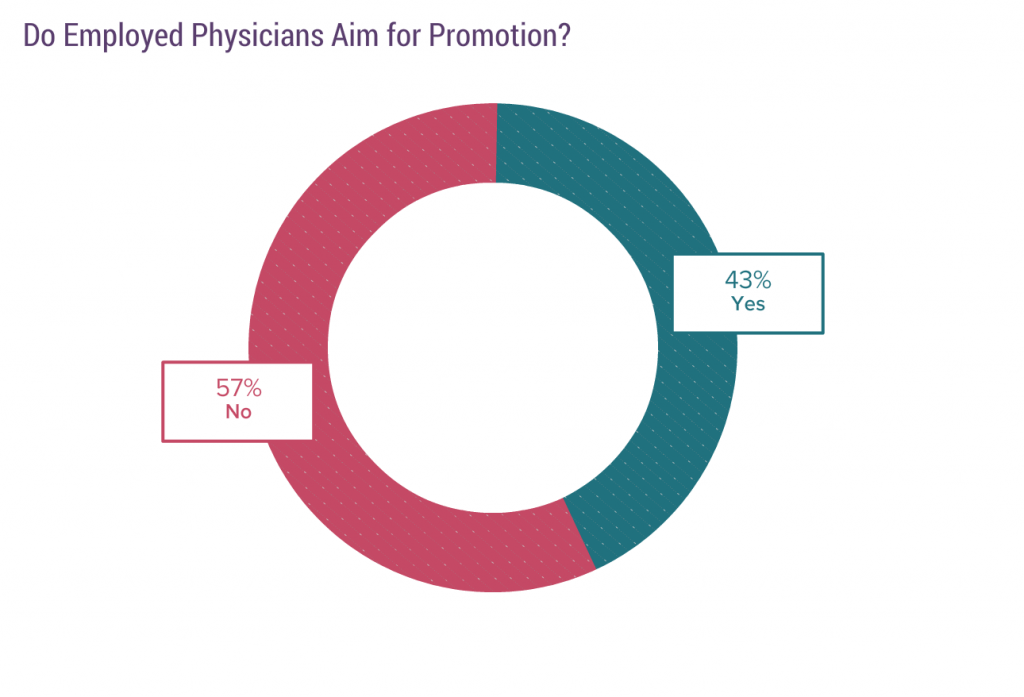
A significant proportion of physicians want a promotion. My interpretation is, they want an escape. An escape from seeing patients (more evidence that being a physician is more of a job nowadays).
And there’s another fact about this:
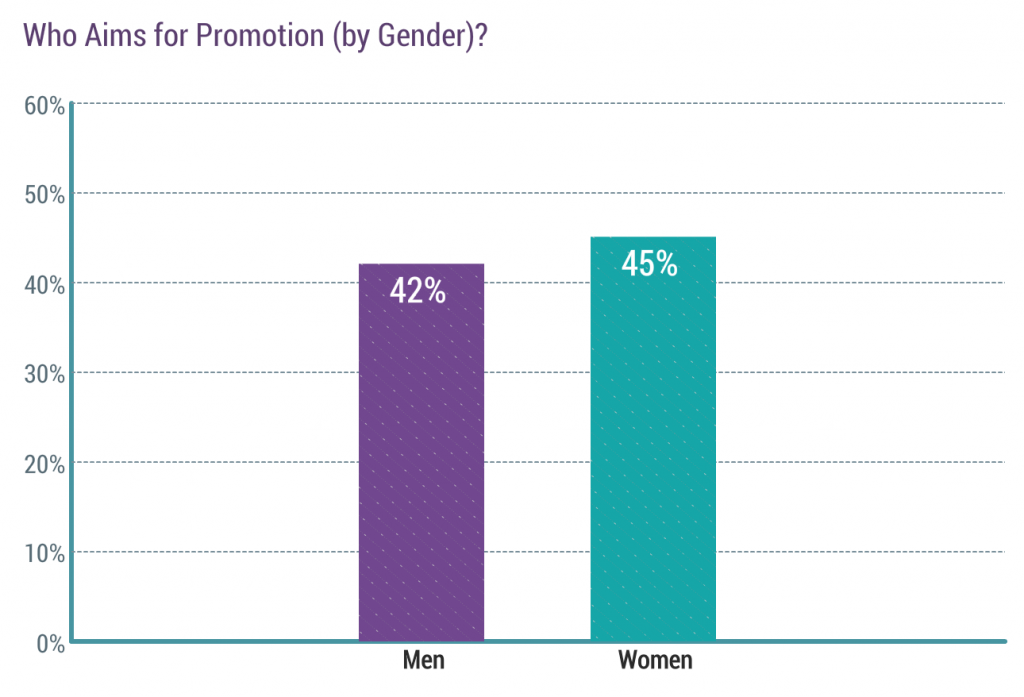
A higher percentage of women want a promotion than men. Probably part of the same phenomenon where women are part time about three times more than men. Child-rearing and lifestyle. Being promoted means more possibility of predictable work hours.
So, what happens is, you have smart but not leadership skilled physicians teaming up with mediocre MBA administrators. Result = lack of leadership, no vision, no real progress.
What you generally get from the non-true leader physicians is a lot of talking. Intelligent talking, but just talking. They haven’t been trained or have the skills to make administrative/operational things happen. It’s parallel to what happens on the clinical floor. Doctor decides something should be done, tells staff to do it. Someone else has to make it happen. Same dynamic. Except on the clinical floor, someone does it. In administration, usually no one does it. So things stay the same and the physicians get frustrated. Then they start to complain. Next, they are asked to step down for being a curmudgeon.
This sets up the classic antagonism between hospital administration and the doctors. You have no idea how many disparaging comments I’ve heard administrators say about physicians in meetings and conversations. When I was the CMO of a health plan with a physician President, we banned any staff member from saying anything negative about a clinician. It would affect every interaction they would have with a clinician. It’s called transference.
So, here is a typical example of how a clinic meeting goes where the staff always defer to the physicians (It’s like a cast system. Talk to any office staff person who has been at these types of meetings.)
Set-up: Physician office with 6 physicians having a monthly all staff meeting before electronic medical records. I.e., everything is paper.
Office Manager: Ok, folks, the docs have an issue related to test results. Dr. Jones, do you want to present this?
Dr. Jones: We physicians have been having a terrible time with test results being filed before we see them. The medical records staff is filing them prematurely. This has to stop.
Office Manager: How many of you are having this problem?
All physicians raise their hands.
Dr. Jones: Well, I know how we can fix this. Starting tomorrow, every test result that comes in must be put into an envelope with the patient’s PCP’s name on it and the envelope has to be stamped with the date. A new envelope per physician is delivered every day. That way, all the test results will be distributed daily. The physician will review the test results, put them back in the envelope and put it in their out box to be filed. Any questions?
Guess what happens the next day? New tasks. No measurement. No one has analyzed the process to see what the root cause was to having tests filed before they get to the physician. This is how physicians “lead”. More of an authoritative manager type leadership.
And most Medical Directorships are filled with non-leader physicians.
Again, Non-leader physicians + mediocre administrators = minimal progress.
Most clinical managers in health care are licensed clinicians who never had any formal management training.
This is really a sin.
Nurses, Physical Therapists, Respiratory Therapists, Radiology Techs, etc. do not get any management training to get their licensure. None, Nada, Nyet. Is it any wonder that health care operations don’t work well, since these folks do become the managers?
Even when you have someone with manager or leader aptitude, health care systems have not invested in adequate management training. What usually happens is a licensed caregiver in a given field is perhaps more passionate or more conscientious than the others in his/her department. There is manager turnover and they promote the conscientious person. Often, they just start their new manager job without any training. Maybe there are some cursory classes they can take. There are never any mentoring programs. These promoted clinicians either sink or swim in their new jobs. If they sink badly, they get fired (a proficient worker now out of the system). If they tread water they are left alone, even though performance is minimally adequate. If they do well, they get promoted again, usually eventually over the limit of their competence (The Peter Principle) but by then, they’ve been around so long, and everyone else around them is a mediocre manager, they maintain their positions. Not much progress. Operational difficulties. No vision. Again.
I hired a person to oversee a non-clinical function in a health plan. She had spent several years as a manager in the banking industry. During her interviews and orientation she related the training programs the bank had put her through. They were very organized and comprehensive. And many hours/days long. I’ve never seen anything in health care that got near what she got for management training. The health care system wouldn’t give her credit for the years she was a manager in the bank when they determined her compensation because “it wasn’t in health care” even though she was the best trained manager I ever hired. Go figure!
Health care management training is woefully inadequate.
I’ve mentioned this before, including the above, so I’ll keep this section short.. Health care training programs for managers are superficial and lack validation from something like the Kirkpatrick Model for proving their effectiveness. As I said before, if there is a “training program” it is some degree of classroom activity (education, not training) with no follow-up and no mentoring program. Then, when a manager has “bad numbers” like low employee satisfaction or financial numbers, they get disparaged by administration and put on corrective action plans, when the corrective action plan should be the administration actually training managers.
Health care management is a task oriented management system vs. a process management system.
I’ve talked about this in previous posts. As in the office staff meeting above, “improvements” in health care systems are usually the addition of tasks that have not been validated or proven to be an improvement. Usually a manager just comes up with an idea and wants it implemented the next day.
[There’s a Quality Improvement saying, “Every improvement requires change, but, not every change is an improvement.” You have to prove that. Some changes make things worse.]
I’ve actually been in high level C-suite meetings where a performance or operational issue came up where a senior “leader” who has no knowledge of the department, its processes or its issues, blurts out a fix and wants it implemented by the next meeting! Not “could we have a diagnostic assessment of what is causing the issue with options for improvement” or anything like that. But it has to happen because he is a senior “leader” giving an order. Kind of a culture of fear issue.
Health care administrations do not understand process at all. They don’t want to take the time to break processes down and redesign them to be efficient and reliable. They don’t understand process reliability or human factors, even though the vast majority of interactions with patients are human to human.
A health care system I was in actually had a person, who was nationally known from a health care “improvement” consulting organization, give a talk about health care process reliability. It was the most superficial, uninformed presentation I have ever heard about the subject. And everyone at the presentation was sooo impressed with the presentation. Just ignorance, really.
If you really want to know about what you need to create and maintain a highly reliable organization with reliable processes read “Becoming a High Reliability Organization: Operational Advice for Hospital Leaders”, AHRQ Publication No. 08-0022, April 2008. Now that’s the presentation that should have been given. I don’t know if any health care system has adopted any of what is in this treatise. It’s almost ten years old now.
The answer to any business/operations problem in health care is: add more people.
This is the result of all that you have read above this paragraph. Since the Health Care Systems’ administrations are incapable of building or redesigning health care processes to be reliable, non-error-prone, or efficient, the only way to keep things together is to hire more people to maintain the workarounds and necessary human effort to over come the inefficient processes so they still, at least, function. Like adding scribes when the EMR is so non-intuitive for physicians to enter information or find things in it. When there is a way to do it (e.g., without scribes) by using available technology and redesigning the practitioner work. Here’s how this could go relative to scribes:
Eliminate the PC in the exam room. No monitor, keyboard or mouse.
Utilize a large Microsoft surface (13-15 inch) or an Apple iPadPro.
The provider wears a headset connected to a real time dictation application, like Dragon.
The provider carries the tablet from room to room. Since most practitioners use 2-3 rooms, there is less cost for hardware since you only need one tablet per practitioner instead of 2-3 PC’s with keyboards and mice.
The practitioner enters the room, introduces him/herself and starts taking a chief complaint and history. In real time, like a pathologist does while doing an autopsy, the practitioner dictates the history, asking the patient if he/she is relaying the information accurately. Then the practitioner does the physicial exam, dictating the findings in real time through the headset. The practitioner then sits next to the patient and they both view the tablet while the practitioner and patient develop the care plan, the practitioner orders any necessary tests, treatment or medications. The practitioner has the patient validate that what he/she has dictated is accurate and that the patient is in agreement with the plan, then discharges the patient in the EMR in real time.
No scribe.
Here’s the final story of this post. Still about throwing people at operational problems.
I’m a VP/Associate Professor of Medicine at a Family Practice Residency Program. The billing office Director comes to our upper management meeting complaining that they are missing the encounter information to bill Medicare, Medicaid and insurance companies for things that the residents did in the hospitals. This was a large amount of revenue lost each month. The President of the program tasks the Dean of Academic Affairs to convene a group to solve the problem. The Dean says he will do that, but he knows how to fix this already. Since I had been trained in Process Improvement in a previous position in another organization, I volunteered to be on the “team”.
We meet a few days later in a conference room. I had invited key individuals that could be involved in the billing for services process. A resident, an attending, billing office folks, etc. The Dean comes in and says, “Thanks everyone for coming, but, this is going to be a short meeting because I know how to fix this. We are going to hire a person to go around the hospital every day and ask the residents what they did that day and fill out encounter forms.”
That was like waving a red cape in front of a bull for me. So, I said, “I’m sorry, we are not agreeing to adding a person until we understand exactly what is going on now.” After a few go-rounds with the team members, the Dean was overruled and we started mapping the current process with a start point at “the resident does something billable” to an end point of “the bill is submitted for payment.”
I won’t get into every detail of the current process or the revised process, as that would be too tedious and long, but, the front end process went something like this:
Every Monday morning the residents had a resident’s report and education session. During that session, on a rotating basis, one of the residents would run around the room and ask the residents what they had done to patients FOR THE PAST WEEK! Now, physicians are smart, but, thinking they can remember every billable service they did for a week was pretty naïve. The resident collating the data had a sheet for each resident which once completed, he handed in to the business office. These forms went through the business office processes to generate bills.
At the same time, residents had to submit proof of their doing certain procedures (like spinal taps) in order for them to meet certification requirements to become board certified. What they were doing currently was jotting these procedure down on scraps of paper or in a pocket notebook with the pertinent patient and procedure information and the date. At the end of the year they would dump this information on the administrative staff to organize and data enter it into a residency program database. This data would be retrievable at time of certification.
We spent two hours mapping the current process. It had swirls and side tracks and tangents. After two hours, it looked so disorganized and bizarre that the whole room burst out in laughter, probably to avoid crying! During the next hour the team devised this new system
A 5×7 “patient card” with all the common service procedures and their CPT codes would be printed in bulk and distributed to hospital wards at the nursing stations.
When a resident admitted the patient, they would stamp a card with the patients hospital card information (they looked like credit cards) and check off the procedures they did at admission.
When the residents had their daily attending rounds the next day, where they presented the cases of all of their patients daily to an attending, they would hand the card to the attending, who thereafter kept the cards in a deck. As the residents gave report on their patients, the resident would recite the services provided during the past 24 hours including the CPT code (this taught the residents CPT coding, an extra benefit!). The attending checked off the CPT codes (the resident never touched the card after handing it to the attending).
When the patient was discharged, the attending put the completed card in a locked box in the daily resident’s report room. Every day at 3:00 PM, someone from the business office would unlock the box and carry the cards to the billing office where the card went through the revised billing office process. At the same time, the procedures required for the Family Practice certification were also gleaned from the same cards and data entered into the programs certification database.
This resulted in three things:
Billings soared! The President was almost gleeful about it.
The residents learned about coding.
The residents didn’t have to independently track their documentation of procedures needed for certification.
The administrative staff didn’t get a dump of procedure information in big boluses once a year.
The funniest thing about this experience was, the Dean didn’t want to present this to the residents. He was convinced he would be lynched by the residents. So, I volunteered to present it. At the end of my presentation they said, “What? I only have the card on day one of an admission?” Me, Answer, “Yes!” Residents, “And I don’t have to keep track of my procedures?” Me, Answer, “No!” The next thing was a standing ovation! The Dean missed an incredible engagement opportunity!
No staff hired…..
Yes, it can be done.
It’s not currently in health care systems’ DNA.
And as another real life example, a recently published article is Health Affairs Blog, a group of folks from the University of New Mexico is convincing people, and has managed to get the NM Medicaid program to mandate hiring and paying Community Health Workers (CHW) to deal with social determinants of health. They report no data that the program actually does anything. Now, I’m a proponent of CHW’s and Promotora’s, but, to disseminate a model and get the model mandated requires some hard data that it is doing something, not just a warm an fuzzy feeling about it, because these CHW’s cost money. There should be quality and financial outcome reporting either included in the article or as a reference in the article. According to the article, the only data they have is the social determinant data they collected. Read ithe article for yourself. Zero validation of it doing anything. And they actually say it’s successful:
“Acknowledging the success of the CHW model, in 2017, New Mexico Medicaid required all managed care organizations to increase their CHW contacts with clients by 20 percent.”
As is usual in health care, they don’t actually report the success other than adoption. Just add people. Push for adoption. Same ol’ same ol’….
Addendum September 21, 2017: Here’s another example. in an article in the Annals of Family Practice (“The Chief Primary Care Medical Officer: Restoring Continuity, Noemi Doohan, MD, PhD, Jennifer DeVoe, MD, DPhil; ANNALS OF FAMILY MEDICINE, VOL. 15, NO. 4 ✦ JULY/AUGUST 2017) the authors propose adding a “Chief Primary Care Officer” to promote improvements in continuity of care and communication across caregivers to improve patient care. So, let’s just add another $300,000 C-suite position to the Chief Executive Officer, Chief Quality Officer, Chief Information Officer, Chief Operations Officer, Chief Medical Officer and Chief Nursing Officer. The first question is, what are all of these other “officers” doing? What is needed is systems improvement not another expensive C-suite Executive. If every hospital system in the country (including “solo” hospitals) hired a CPCO, as these two naive MD-PhD’s propose, the cost to the US would be around one billion dollars, using $250,000 as a salary and benefits estimate. Really? How about spending that on designing reliable health care processes.