
Why The United States Health Care System Costs So Much – Part Six – Administrative Costs
Berwick and Hackbarth define Administrative costs thusly:
“Administrative Complexity: the waste that comes when government, accreditation agencies, payers, and others create inefficient or misguided rules. For example, payers may fail to standardize forms, thereby consuming limited physician time in needlessly complex billing procedures. We estimate that this category represented between $107 billion and $389 billion in wasteful spending in 2011.”
As you can see, Administrative Complexity is the biggest wedge in this graph. In actuality, you should add Administrative Complexity and Pricing Failures together to get Prices (Berwick and Hackbarth’s definition of Pricing Failures has to do with the perverse “market forces” only, i.e., “the waste that comes as prices migrate far from those expected in well-functioning markets”. See my post on Prices, in which this is all inclusive.) I say this because the health care providers have to make their profit margin expectations and they are funding resources to manage the administrative complexities in the US health care system which drives up prices.
So, what makes up Administrative Complexity? Well, you can divide this up into three categories:
- Health Insurance complexities
- Government laws, regulations/Legal and Compliance
- Health Care Provider “internal” rules and policies
Let’s go through each of these.
Health Insurance Complexities
This is my favorite pet peeve, and I worked in several health insurance companies. As a physician executive in those health insurance companies, I did everything I could to minimize the administrative burden to members (patients in insurance speak) and health care providers.
Here’s what those companies foist on members and providers:
Company specific rules
Prior authorizations
Notifications
Eligibility procedures
Billing procedures
NOTE: Every insurance company has different rules about these. Trying to keep up with them all is an administrative nightmare!
Company specific rules
Each insurance company has “rules” they want the health care providers (herein called providers) to follow as a provider in their network. These are laid out either in the contract between the insurance company and the provider or in the provider handbook. The rules described in the contract usually require a notification period (defined in the contract) for changes, but, a lot of the handbook rules can be changed at any time by the insurance company. The provider can’t change any rules; it’s a one-way street.
Here’s an example. An insurance company had a rule allowing the Medical Director of the hospitals in their network to call the insurance company Medical Director and discuss inpatient cases whose admission, or some days of the admission, had been denied by the insurance company (herein called health plan). Often, the health plan had incomplete information about the admission and a five-ten minute conversation to their Medical Director and faxing some additional information caused the Medical Director to approve the admission or denied days. One day, without warning, when the hospital Medical Director called the health plan to discuss a case, he was told the health plan changed its rules and would not be allowing the hospital Medical Directors to speak to the health plan Medical Directors, and, if he wanted a reconsideration of a case he had to file a formal appeal. Filing a formal appeal was time consuming, required a series of administrative steps with the health plan, photocopying dozens of medical record pages, etc. This added even more administrative costs to the hospital AND the health plan. The health plan was OK with increasing their additional costs because they know that hospitals will not file formal appeals for a certain percentage of cases because of the workload to file them, and that the health plan would be more likely to uphold the first denial decision using a non-person-to person appeal process. The money saved because of these two things is way more than the salary and benefits of a couple of FTE to manage the extra work.
Members are also subject to health plan rules. If you are in a health plan, you have gotten a member handbook and a “summary of benefits” which are just like in that Libery Mutual car insurance commercial where the woman says the page in her handbook says “blah, blah, blah..” Have you read every page of your member handbook? If you did, did you understand it all, or, are you sure your interpretation of the rules is the same as the heath plan’s?
The one that is most irritating to members is when they get referred to a specialist or a testing facility that is not in the health plan network by a PCP, or when they are referred to an in-network provider but the PCP doesn’t know she has to file a prior authorization for the service with the health plan. The member gets a denial for the service and the bills. For members, rules changes by the health plan usually require, by state or federal regulations, advanced notification. However, these are usually letters sent to members about things they haven’t experienced yet and they forget about the letters. If a member doesn’t like the denial, they have to file a formal appeal, which is just as labor intensive for the member as the hospital scenario above.
All of this adds costs to the system.
Prior Authorizations
Both providers and members hate these. They are a foundational function in any health plan.
There are two kinds of prior authorizations (PA’s), medical necessity and administrative.
For Medical Necessity, the stated reason by health plans for prior authorizations is to make sure providers are practicing according to best medical practices. For some prior authorizations, that’s actually true. Health plans usually have “Medical Policy” committees that review literature and they contract with proprietary companies that have physicians on panels that review literature and offer opinions and recommendations (Winnifred Hayes for example), and they usually get the opinion of an in network physician, then they promulgate a policy. An example would be a prior authorization for bariatric surgery (you know, those surgeries obese people get so they can lose weight). You have to be overweight by a certain amount, and ascertain that you have an obesity related complication, like diabetes, etc. This would all be based on the medical literature’s recommendation of who should get this type of surgery.
This is all well and good except there are sometimes circumstance that aren’t defined in the literature that should be taken into account. Remember in one of my previous posts when I talked about the “bell curve”, that people and the way things impact them isn’t identical for every person? Well, this is also operative with PA’s. Some health plans are more flexible about this than others. Only a Medical Director can make a medical necessity denial and it is considered by most states that Medical Directors doing PA’s are practicing medicine and have to be licensed in the state where they are making these denial or approval decisions. They can actually be sued for malpractice related to their making health plan medical necessity decisions.
Another problem with medical necessity policies is, there are often financial reasons for the wording in medical policies or in their implementation. That’s why, if you looks at several health plan medical policies for the same procedure, they will have different approval elements, even thought the literature is the same.
That’s because the real first reason for PA’s is not to make sure the providers in the network are practicing according to best practices, but to save the health plan money.
And the administrative burden for PA’s is quite high. Obviously, health plans have dozens of staff, mostly nurses (who have been sucked out of the health care caregiving systems) processing PA’s all day long. Provider offices always have a person trying to run down prior authorization processes. The PCP has one trying to generate them and the Specialist has one trying to make sure the authorization has been approved before the patient arrives or when they arrive.
And health plans often just apply the PA’s to hassle providers and members enough that they don’t want to go through the effort of getting a PA. So, whether the patient needs something becomes a moot point. The administrative burden to request a PA results in a deferral of the patient getting the service.
The other PA is called an Administrative PA. This is when the contract between the member and the health plan specifically says something is not covered by the premium the member is paying. These things are variable by health plan. An example would be, cosmetic surgery is not covered under the health plan contract. If a member or provider requests coverage of something cosmetic, the denial doesn’t require any type of supportive medical literature. The member simply didn’t pay for cosmetic procedure coverage. A non-physician can make administrative PA denials since there is no application of medical necessity. Of course, members and providers will still appeal administrative denials, which is labor intensive and requiring provider and health plan resources, adding to costs.
Here are some true stories about PA’s.
This first one is interesting because it ended up the member agreed with the final outcome but the provider didn’t.
A request came across my desk from an Oncologist to have a patient with gastric cancer to go to a major distinguished cancer center for a Phase 2 clinical research trial. A Phase 1 trial determines if the new treatment is safe. A Phase 2 trial determines if the new treatment does something positive (you don’t know it is positive or negative until the end of the trial). A Phase three trial determines if the new treatment is as safe or safer and the same or better than the current standard of practice. Health plans generally don’t cover Phase 1 or 2 trials. This is because they only want to cover things that have a known beneficial effect on a person and you can’t say that for Phase 1 and 2 trials. Plus, it’s a way to decrease medical costs.
Anyway, I got this request. I called the Oncologist who strongly advocated for the patient getting the Phase 2 trial covered. His main selling point was, the patient was relatively young, had a treatment resistant cancer, hadn’t responded to standard therapy and should have a chance to get whatever treatment is available, whether one knew it worked or not. This position actually violates the bioethical principle of beneficence, which, summarized, says a doctor can’t offer a treatment to a patient unless the net benefits to the patient outweighs the harms. You can’t say that for a Phase 2 trial. You have no idea how many conversations I had with Oncologists about this. They just wanted their patient to get something whether it was proven or not. Like I said before, most health care providers don’t understand bioethics.
I then called he patient. His Oncologist had convinced him he should have the treatment in the Phase 2 trial. I asked him if he minded if I called the principle investigator of the trial to get more information. He said that would be fine. I told him I would call him back with what I found out.
I called the principle investigator. He was a really nice guy. He described the protocol to me. It was a three drug combination given over 24 hours in an IV drip. I asked him how many people were in the trial and did he have any preliminary outcome data. He said the patient in my health plan was only the fifth person to be enrolled so he had no data yet. I asked him if there was a study that preceded this one using the same drugs. He said there was! The previous study gave the drugs in an IV bolus (pushed with a syringe over several minutes). I asked him how that study turned out and he said they stopped the study because the patients were dying faster from the treatment than the disease. (See what I mean about Phase 2 trials?) He said they thought if they gave the same drugs in the same doses over 24 hours, they might help without killing people.
I thanked the research physician for being so transparent about his research. I called the member and relayed exactly what I had heard. He immediately said, “Please cancel my request, I don’t want to take that chance.”
This is one reason why there are PA’s.
On the other hand, here’s a Pharmacy one that is the opposite. People get fungus in their toenails. You’ve seen ads about that on T.V. It’s considered cosmetic. It just looks bad. The standard treatment was griseofulvin, an oral antifungal. Griseofulvin has a fair amount of adverse effects including liver dysfunction, requiring lab test monitoring and you have to take it for at least 6 months for it to be effective. In 1996, terbinafine came out. It had fewer side effects, reduced required lab testing, lower incidence of liver dysfunction, and you only had to take it for 12 weeks. The health plan pharmacy department designated terbinafine as requiring a PA which stated the patient had to have an immunocompromising condition, like diabetes or HIV, and the fungus had to be causing a significant irritation to the skin or a bacterial infection in the skin adjacent to the nail. All other requests were considered cosmetic, the nail just didn’t look good. This made the PA a medical necessity PA.
There was NO PA for griseofulvin. That meant a doctor could prescribe it for any toenail fungus infection in any person and without any sign of irritation or infection! The real reason terbinafine was under a PA was BECAUSE IT COST FIVE TIMES WHAT GRISEOFULVIN DID (griseofulvin being generic). No matter how I pressed the pharmacy department pharmacists, they wouldn’t admit that the PA was strictly to save money so they could meet their pharmacy budget drug spend target.
PA’s require appeals processes. There is usually a first level, where a Medical Director decides upholding or overturning a denial, a second level appeal where a health plan Appeals Committee, consisting of health plan staff, who vote to uphold or overturn the denial, and a state Department of Insurance (DOI) Appeals Committee where persons hand-picked by the DOI decide. A state Appeals Committee may have physicians or not on the committee. Sometimes the committee is only citizens with no medical background. With the state committee, it is funded by your taxes! More money going to health care administrative costs!
Bottom line for PA’s: There are good PA’s and there are bad PA’s. You won’t know the difference. If you really think you need something, appeal, appeal, appeal!
I always tried to implement things to minimize the burden on providers and members regarding PA’s. The Finance guys were very resistant to reducing PA’s or making it easier for providers to obtain PA’s (The rationale for the latter is, the more work a provider has to do to request a PA approval, the less likely they will ask. This, of course, keeps the health plan’s medical costs down).
Here are some of things I did in health plans that were pretty much reversed after I left, usually because the Finance guys put pressure on my predecessor.
To determine if you are actually getting cost savings from a PA, you have to have a net cost reduction according to this formula: Amount of money saved with a PA – the administrative cost to do the PA = a positive number. Otherwise, your costs are higher due to excessive administrative costs.
Here’s an example. If it costs $50 on average to process a PA and only 1% of the PA’s are denied, the service with the PA has to cost $5000 for breakeven in the formula above. If the procedure costs less than $5000, you’re wasting administrative dollars.
I had my Vice President of Medical Operations do this calculation annually. If the result was a negative number, we discontinued the PA. This freaked out the Finance guys because they said the Hawthorne Effect was causing the 1% denial rate (the Hawthorne Effect is: when you are watching someone they are more likely to “do the right thing”). To offset this rationale we monitored the frequency of the services every six months. It was rare that they increased. When I left that health plan, they re-instituted all of the PA’s we discontinued, and their costs didn’t go down.
Another thing we did was, we set up a website where the criteria for PA approvals was displayed by PA. The provider would check off which criteria had been fulfilled and checked another box stating that the information provided was true and if not the provider would be subject to fraud charges. If the criteria were met, the provider got an immediate PA approval online. They loved this! Within six months of my leaving that health plan, the website was inoperative. Back to the faxing of PA’s! More money spent on administrative costs!
Notifications
Notifications are when a provider, usually a hospital or ER, has to notify the health plan within a set amount of hours that a health plan member was admitted there. It has nothing to do with a PA. If you don’t notify the health plan within the specified time frame, the bill sent to the health plan is denied, the provider loses the revenue for that service.
This is essentially an administrative hurdle that health plans know a service provider can’t meet all the time. As a matter of fact, for most notifications, a service provider only meets the time line at most 90% of the time. A health plan can reliably predict they will save 10% of the costs for those services if they implement a notification rule. They often do this without warning. Even if they warn you, they give you a short lead time, knowing you can’t gear up for the notification overnight. I saw this in action in every health plan I was in.
Notifications are simply tactics by health plans to save money. But they cost money in administrative costs, especially to the providers trying to avoid a denial. The health plans just have a computerized edit in their IT system, so it doesn’t cost them much if anything.
Eligibility Procedures
Every time you see a health care provider, they have to check with the health plan to make sure you are a member and you have the needed coverage. More work and cost for the provider.
Billing Procedures
This is obviously sending a bill to a health plan. Nowadays most bills are sent electronically. The bills have to be processed by a “clearinghouse” company, which costs the provider money. The billing requirements can also be different among health plans which can cause confusion, rejected bills, etc. The providers usually challenge any billing rejections, which means there is a department and set of processes for that at the health plan. Just another opportunity to increase costs.
Government laws, regulations/Legal and Compliance
This administrative complexity group has become quite onerous. There are federal and state laws, Medicare and Medicaid regulations (for Medicaid there are both state and federal, Medicare is federal), Department of Insurance (state) regulations, The Joint Commission (accreditation) standards, NCQA (for health plans, etc. It’s especially onerous for hospitals, who have entire departments dedicated to maintaining compliance with all of these entities. Just keeping track of all of the requirements is daunting. There is usually a VP of Compliance, compliance officers, and the largest portion of the Quality Department (another reason Quality is #4), all dedicated to this effort.
And then, there is the site visit. Each government agency or accreditation agency will come and do a site visit, where they spend up to a week combing through the hospital or health plan looking for “deficiencies” or “findings”. If a hospital gets a warning with lead time that a site visit is scheduled, they stop all work except direct patient care and focus on looking for deficiencies and either fix them or hide them before the site reviewers show up. This delays any implementations or improvement projects. The delay is longer if there are significant “findings” because these have to be fixed within a certain period of time, like 90 days, with the regulator or accreditor doing a follow-up site visit to ensure things were actually fixed. Time virtually stops at hospitals until the second site visit.
Health Care Provider “internal” rules and policies
Health care systems, for some reason, like to impose rules on themselves that increase their administrative costs and burden. This always seemed weird to me since they had enough external rules and regulations to deal with.
There are several reasons for this category:
1. Either administrators or doctors dictate a task or a process without analyzing the impact. They just pile on one task on top of another. Soon, the administrative work gets in the way of taking care of patients.
Here’s one showing how rules get in the way of taking care of patients. At a medical group in which I saw patients, there was the “ten minute rule”. If a patient was ten minutes late for any appointment, they had to reschedule. They were pretty strict about this. They weren’t concerned with what patients were going through or why they were coming in. Maybe their baby had a diarrheal BM just as they were getting in the car. Maybe they had a flat tire. Maybe the traffic was horrendous. Didn’t matter.
FYI, I never followed this rule unless, when I was a PCP, a patient was a chronic no-show or always came late. Then we warned them that if they came late and their problem wasn’t acute, they would be rescheduled.
I was seeing same day patients in a clinic when the receptionist came back to tell me a patient was over ten minutes late and did I want her to reschedule. I said, no, tell her I will see her, but she might have to wait a little bit. The receptionist left. My nurse said, “You should make her wait at least an hour before you see her.” I said, “Why would I do that?” She said, “ You should punish her for being late.”
WHAT?!? Punish a patient?
This rule got in the way of taking care of patients. Who knows what might happen to them between the day they were asked to reschedule and the rescheduled day.
2. The Legal Department or Compliance Department institutes tasks or policies to “minimize legal risk”. Most of these raise provider administrative costs.
Here’s a couple.
In any state I’ve practiced, an Advance Practice Clinician (Nurse Practioners, Physicians Assistants) can see patients without a physician present as long as there is some formalized oversight process. In one health care system I worked in, the legal department pushed the rule that a physician must be on site for an APC to see patients. This really played out negatively in Urgent Care. At one point, they didn’t have enough doctors to man the Urgent Care (UC) centers for all the times the UC center were advertised to be open. This resulted in the UC centers closing at times. This rule increased administrative costs (because the higher priced physician had to be present) and they lost revenue when there weren’t enough physicians.
Here’s another Urgent Care one.
In all of the UC centers at one health care system, all of the doctors and APCs had to be Advanced Cardiac Life Support and Pediatric Advanced Life Support certified (ACLS and PALS). These certify practitioners to run Codes (like Code Blue’s). This alone cost money because, since it was required, the UC centers had to pay for the certification courses. These are every two-year certifications. The UC center didn’t run mock codes to keep practitioner skills up. There were rare Codes in the UC centers. Some practitioners who had been there for years had never run a Code. The literature says just doing high quality Basic Life Support (BLS) until a patient gets to an ER has better outcomes than doing codes in the field. Plus, because there weren’t many Codes in the UC’s, the drugs in the crash carts expired and had to be thrown away and replaced with new drugs (costly). Since we were in a big city and the ambulance response times were less than 10 minutes, it was possible to discontinue ACLS and PALS, train staff in BLS and remove the crash carts from the UC centers saving a ton of money. As a matter of fact, when I was in a different state, our legal department advised us that we could do that, and we did.
And here’s validation for ambulance response time. Here’s a table from a study that determined ambulance response times in urban, suburban and rural areas:
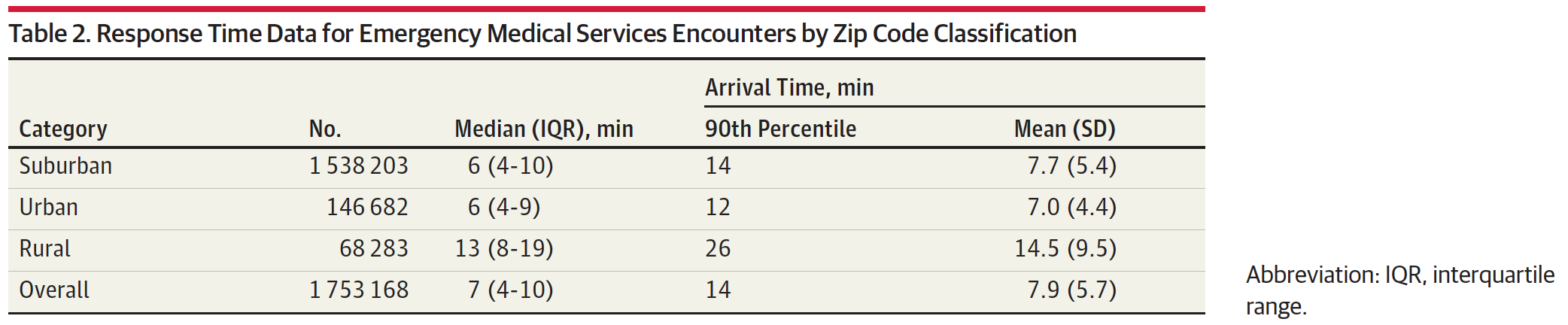
The median response time is six minutes and the average was seven minutes for urban and suburban (we were in urban). The worst response times were 12-14 minutes in urban and suburban.
The Legal folks for these UC centers would not even give an opinion about discontinuing these things. Their stance was, it was better to keep doing what was being done. After all, the providers were certified, weren’t they? I’m sure I could have shredded their argument in a court. Me, “Doctor, when was the last time you had to run a Code?” Doctor, “When I was in training.” Me, “Never at the Urgent Care Center?” Doctor, “No, sir.” When was the last time you participated in a mock Code at Urgent Care?” Doctor, “Never.” Me, “What dose of epinephrine do you give a 3 year old with V-fib?” Doctor, “I don’t know, I’d have to look it up. We have posters on the wall of the procedure room to remind us.” Me, “What if the patient is not in the procedure room?” Doctor, “Uh, I dunno. Ask a nurse to run there to find out?” Urgent Care settles out of court.
I’ve had compliance officers tell me I should make my staff do things they were saying we must do because “it was a reg” (a regulation). When I read the regulation, it said nothing like what they wanted me to make my staff do. When I showed them the regulation language and said, “It doesn’t say what you are saying”, they would say, “Well, but the regulator’s intent when they were voting on this was what I told you”. I would say, “Were you there when they voted?” they would say, “No, but I know how they think.”
What?!?? The compliance officer is a mind reader?
Every time this happened I eventually got to actually asking the regulator to validate their regulation, including the “intent”. 100% of the time, it was exactly what the language said in the regulation, not what the compliance officer was advocating. If I just went along with the compliance officers, I’d have increased administrative burden on my staff for no reason. And add administrative costs to the health plan’s premiums.
This one story is even worse.
According to DOI regulations, if a health plan denied a medical service in process, like a patient is getting physical therapy visits and the concurrent review nurses advise the Medical Director that the case doesn’t meet medical necessity requirements anymore, then the member had to be notified in writing that further Physical Therapy visits would be denied. At the same time, as a value-added service (purportedly, to reduce health care costs) health plans offered Case Management services to members, which is not considered a medical service, it’s an administrative service. A compliance officer was talking on the phone to a staffer in the DOI who was a member of our health plan. and had been in case management. As is typical of case management, when the person met their case management goals, their enrollment in case management was discontinued, which was relayed to him verbally on the phone. He told the compliance officer that it would have been better if he had also gotten a letter. The compliance officer came to my staff and told them they had to send letters to members when their case management was being discontinued, that the DOI had told her we must do it. This would have added administrative costs. I de-bunked that one, too. There was no DOI requirement that we inform members who are discharged from case management in writing. We didn’t do it.
You have no idea how many times the legal and compliance folks convinced the administration that we had to do something we didn’t have to do to the point that it interfered with getting business goals accomplished, with no credible foundation for their opinions. This is another flaw in health care administration. Because health care administrators are usually C-players (subject of another post), they defer business decisions to their lawyers, which should never happen. Lawyers are called “counsellors” for a reason. They are supposed to counsel business owners on the risks, “loopholes”, etc. in the laws pertaining to the business situation at hand. A business owner should always make the business decisions. Never lawyers.
Needless to say, the compliance and legal folks didn’t like me.
But I did minimize administrative costs for the health plans, our members and our network providers. Too bad it never lasted after I left.