
Why The United States Health Care System Costs So Much – Part Four – Overtreatment – Technology
Here’s the post about one of the two main drivers of US health care costs. The use of technology. More than most other countries. The main offenders are:
- CT Scans
- MRI Scans
- The Da Vinci Robot
Before we get into the specific pieces of technology, here’s some background information.
Back in “the day” (before 1990) Medical Students and Interns and Residents in training were trained differently. CT scanners started to be installed in hospitals in the mid-1970’s but were very rudimentary (for example, until the early 1980’s you could only do a CT scan of the head because the speed of the CT scanners were so slow that any movement, like breathing, would blur the image). It wasn’t until about 1985 that most parts of the body could be scanned. The first MRI machine came out in March of 1980 and its dissemination took about ten years. So, before 1990, a doctor had to rely on looking at the patient (history and physical exam), analog x-rays, and blood/fluid tests. After 1990, Med Students and residents began to rely on the emerging technologies to “examine” the patient. Kind of like Dr. Leonard McCoy (Bones) on Star Trek who used a tricorder (hand held diagnosis device) and the electronic headboard in the Starship Enterprise. Touching patients, feeling for abnormalities, observing patients and talking with patients started to take a back seat to CT scans, MRI scans, and more diverse and available blood tests. Admixed with this was the advent of the Electronic Medical Record (EMR), which recent studies show, has reduced the time practitioners spend with patients. The most recent article showed a practitioner spends 50% of their time actually seeing patients and the other 50% of the time “on the EMR” either reviewing information or messaging patients and other practitioners, while spending the same amount of time in their offices. Main result, much less patient contact time.
This phenomenon has caused concern. In a recent JAMA Internal Medicine issue there is an article describing this (Hiding in Plain Sight—Resurrecting the Power of Inspecting the Patient by Shlok Gupta et al, June 2017). Here’s an excerpt from that article:
“An unintended consequence of deriving information from the electronic medical record instead of the patient, however, has been an atrophy of the powers of clinical observation. Inspection is a diagnostic, prognostic, and humanistic tool, as we have learned from our patients and teachers over the last 4 decades.”
Here’s a real/true example of the atrophy of observational skills, of being aware of what looks normal and what looks abnormal:
There was a patient in the hospital who had several conditions. One was an infection, so the hospitalist team started the patient on antibiotics. The patients’ white cell count came down but he continued to run a fever on the fourth day in the hospital. The hospitalist team did another fever workup and added another antibiotic. After three more days, the patient still had a fever. Stymied, the hospitalist team requested an infectious disease (ID) specialist consult.
The ID specialist, who was my age (that is, an “older guy”), reviewed the record (which showed a sustained linear fever without much fluctuation), talked to the Hospitalist, and then did a history and physical (which was unremarkable for findings of an active infection). But the key observation was, the patient was sitting up, smiling, looking perfectly normal, not complaining of anything. To the ID Specialist, this was a dichotomy. But, he had seen this many times before, because he had spent so much time with patients. His diagnosis was a drug fever, most likely from the antibiotics. The patient was taken off of his antibiotics and his temperature was normal within 36 hours. He blamed the hospitalist team’s “atrophy of observation” as the cause of this patient’s extended stay and the cost of the ID consult. They were stuck in the EMR temperature chart and not looking at the patient and processing what he looked like.
So, because of the combination of the “I can get a test to figure that out” thinking instead of “touching, listening, feeling”, and the reliance of the EMR, practitioners are now “addicted to the test” and not paying attention to YOU!
This has resulted in increasing usage of CT and MRI scans. Why take the time to examine someone? I can get an image! The problem is, not all things can be seen with a scan. You can’t see bacteria circulating through a patient’s system. You can’t see something that is “functional”, only “anatomic”. I can’t tell you how many times I’ve seen the younger generation doing a test when there was an obvious physical finding. I had one patient in Urgent Care who had been to two ER’s, got scanned at both and was told they couldn’t find anything. I examined him and within 5 minutes had the correct diagnosis. He was stunned and said no one had examined him that way, why was that? I told him I didn’t have the scans when I was trained so I rely more on the history and physical. His problem was functional. He recovered.
Here’s another one. This one is really scary, so fasten your seatbelt!
It’s Thursday afternoon. I’m seeing same day patients in a primary care clinic. A man in his 60’s come in with a complaint of right arm pain and numbness. He had been to the ER three days earlier. They did an MRI, which showed a bright lesion in the cervical spine, the brain was normal. They told him he had a Transient Ischemic Attack (TIA) (a “mini-stroke” that resolves).
First, pain is not a typical symptom of a stroke. Second, if it was a TIA presenting with pain, a TIA “resolves” so the pain should be gone. A stroke should be farther down the list. He described the pain as excruciating, kept him up at night despite pain medicine. He thought his right arm was weaker than the left and somewhat numb.
On physical exam he had a mild upper extremity only weakness, pinprick exam seemed to aggravate his pain. But the key exam finding was: he had a positive Lhermitte’s sign. This is caused by a lesion in the neck (cervical) spine or the brain stem. It is common in Multiple Sclerosis and Transverse Myelitis, which are irritative lesions. Strokes are “ablative” usually, meaning a piece of your nervous system dies. And TIAs don’t typically occur in the cervical spine. I think the ER practitioner was looking more at the brain and not at the cervical spine and seeing nothing in the brain, called it a TIA (just my assumption). The “sign” itself occurs when you bend the patient’s neck. They get the feeling of an electrical shock going down their back, often into the legs. Interestingly, when I relayed this case to the younger doctors who worked in the medical group, none of them had heard of a Lhermitte’s sign. I wasn’t surprised.
Well, he had this Lhermitte’s sign. That coupled with the bright lesion in the cervical spinal cord on the MRI, had me strongly suspecting transverse myelitis. I didn’t have admitting privileges and wasn’t sure he would do well with a blast of outpatient steroids, so I called our medical group’s neurologist. It was 4:30 PM on a Thursday. (Remember what happens nowadays at 4:30 PM in doctors’ offices? Remember the story about the post-surgical patient who was sent to Urgent Care when he called his surgeon at 4:00? Yup, they’re GONE for the day). I got the neurologist’s nurse, told her the story, told her my concerns and that I wanted to speak to the neurologist as soon as possible. The nurse said the soonest she could give the neurologist the message was the next morning. I told her I wanted to hear from her before noon, please.
I sent the patient home, telling him we would be calling him about seeing a neurologist ASAP. The next day (Friday), I didn’t hear from the neurologist by noon so I called again. The neurologist was out at lunch and couldn’t be contacted. The nurse told me the neurologist asked her to schedule the patient for a Nerve Conduction Study the next Tuesday WITHOUT EVER SEEING THE PATIENT! And, I’m guessing, she didn’t look at the MRI. Yes, she was relying on a test. I said that was unacceptable. I had to speak to her. Please have her call me today.
I was really busy that afternoon and I didn’t get around to calling the neurologist back (because she never called me!) until 4:30 again. Unfortunately, same result, neurologist was gone and still wanted the Nerve Conduction Study, not a call to me or an appointment with the patient.
At this point, it is Friday at, now, 4:45 PM. I got more assertive with the nurse, telling her I feared for the patient and really needed to speak to a neurologist. I didn’t want to send him back to the ER where they misdiagnosed him; I figured he’d get the same diagnosis. The nurse said, “Well, there is a locum tenens (“rent-a doc”) neurologist hospitalist. Would you like to speak to him? I have his pager number. He’s about to go off duty at 5:00 PM (meaning there would be NO neurologist to talk to after 5:00!).
I got his pager number and immediately called him. Thankfully, he called me back in five minutes. I got about halfway through my story and he interrupted me and said, “This guy needs admission and high dose IV steroids for at least a week! Get him to the ER now and I will take care of it! Hopefully his lesion isn’t progressing because if it does, it’s at a level where he could become quadriplegic and stop his respirations!” (Just like Christopher Reeve!!!)
OK, now I have a plan, but no patient! I was not at the clinic where I saw the patient. It was now 4:55PM. We didn’t have an EMR at the time. I had no contact info for the patient. I called the clinic where I saw the patient. The pod clerk was still there. I told her what was happening, we had to get in touch with this patient.
It took us until 6:30 PM to finally track him down. (I stayed at work by my phone, calling the pod clerk every 15 minutes for an update.) His wife was away, he was alone (not good given the possibility cited above) and he was out walking his dog during the 90 minutes we were trying to find him. The pod clerk was AWESOME; she never gave up! (Remember on my front page when I listed who really cares about the patient!?)
The patient made it to the ER, got admitted and was on high dose IV steroids for 7 days then discharged on high dose oral steroids. Eventually the transverse myelitis resolved. Whew!!
The next week, when I went to the clinic, I hugged the pod clerk and thanked her profusely. She said, “I want you to be my doctor. I don’t know anyone else who would have done what you did.”
Well, I don’t know if that’s true, but, the neurologist was doing the “I can just do a test to figure this out” routine, wasn’t she?
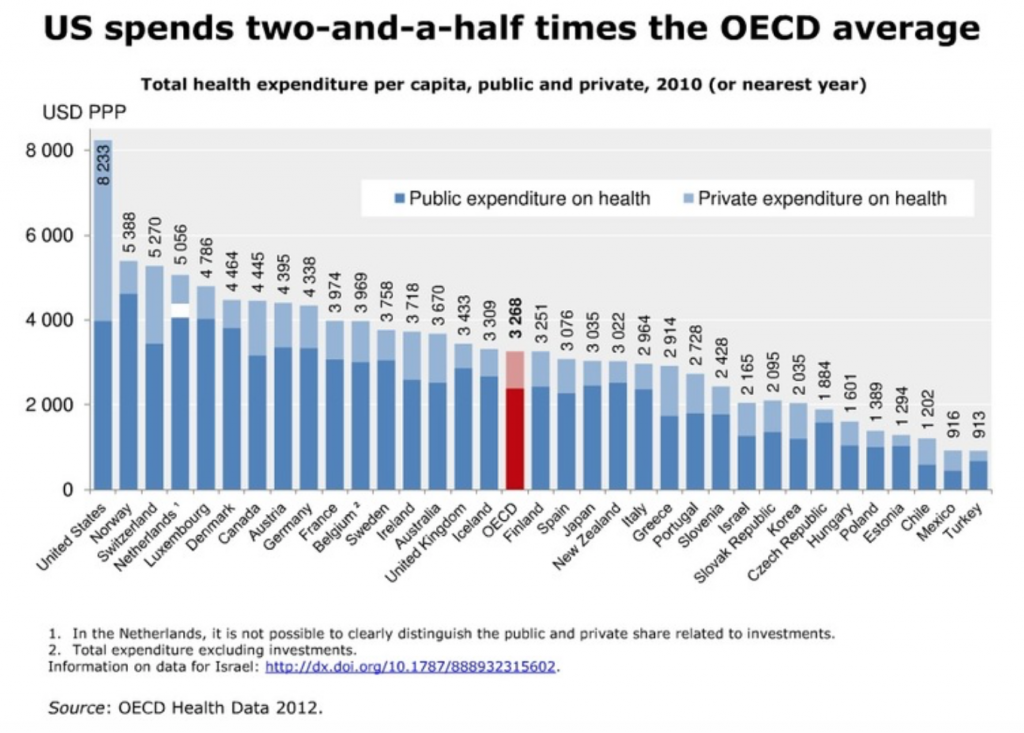
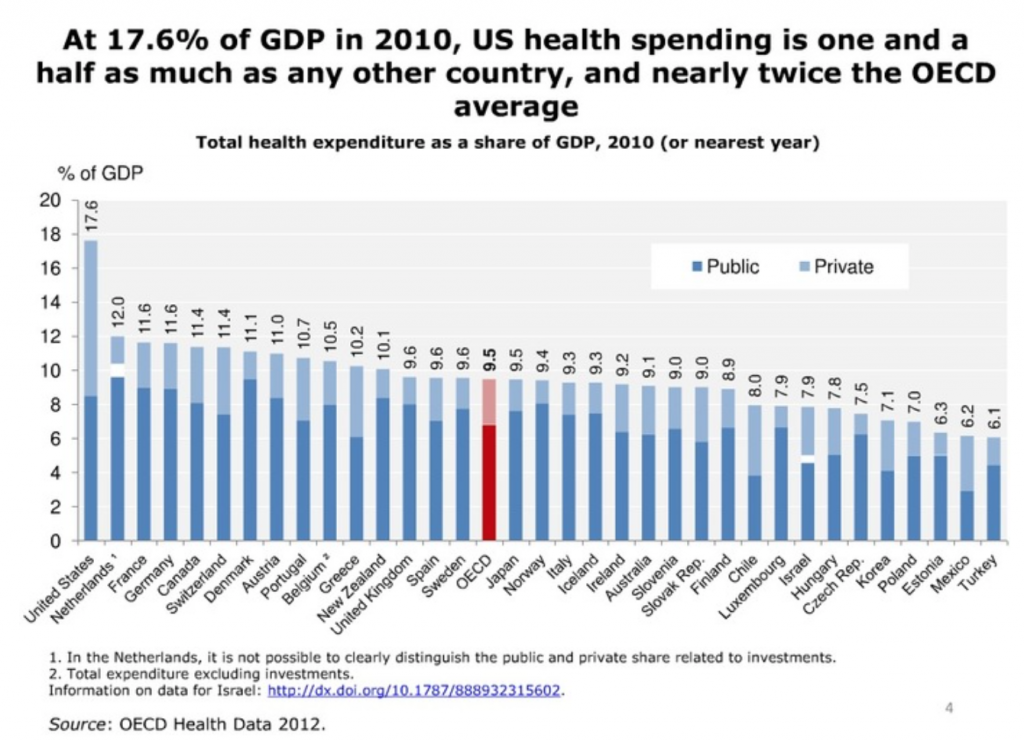
OK, now back to the analytics of CT scans and MRI’s. Here are some graphs explaining the problem. Remember in the USA, these tests are often many times the cost in other countries. The below is all OECD (The Organisation for Economic Co-operation and Development) data:
Review of health care spending by country
Use of CT scanners and MRI
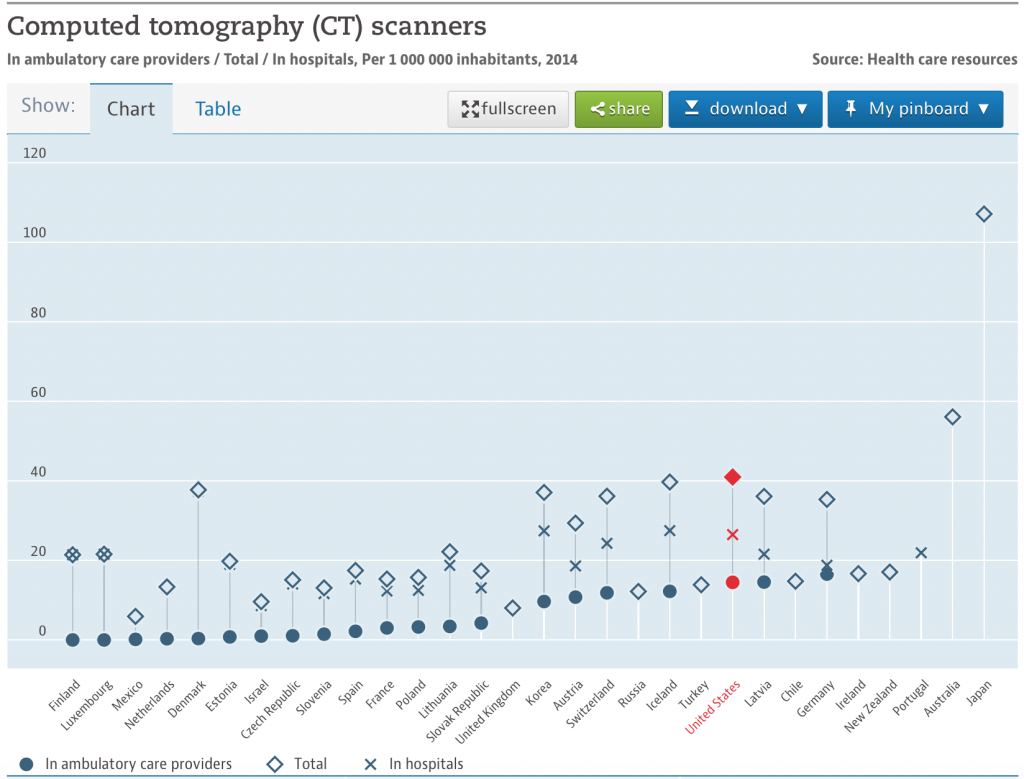
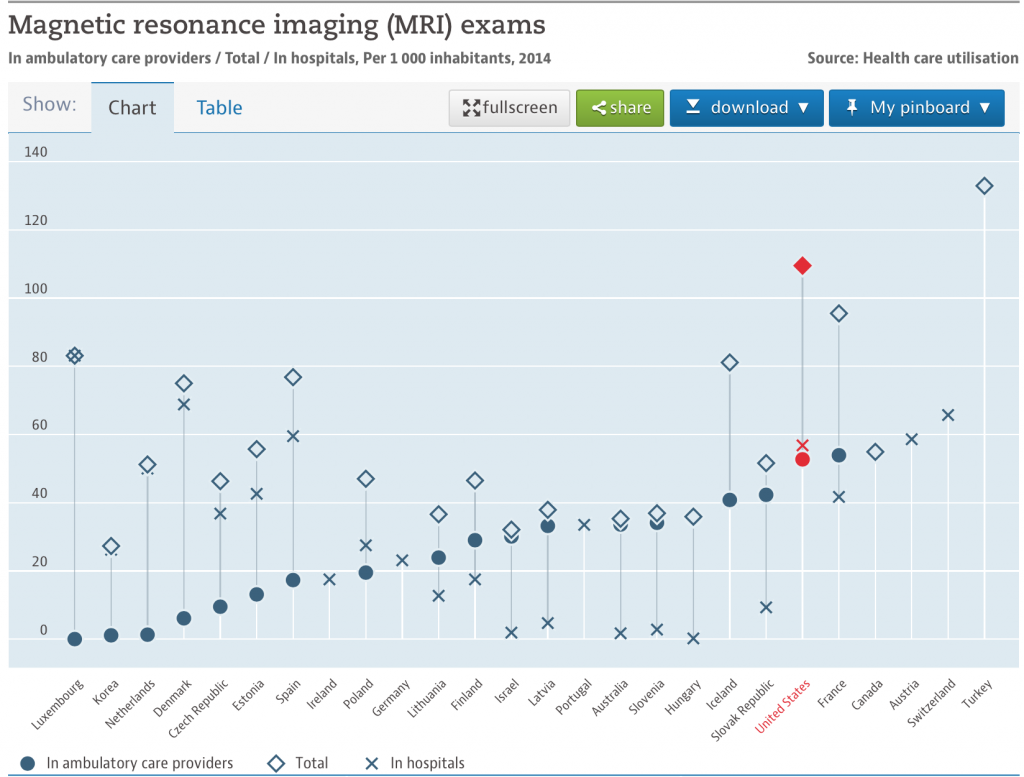
Here are the unit cost numbers:
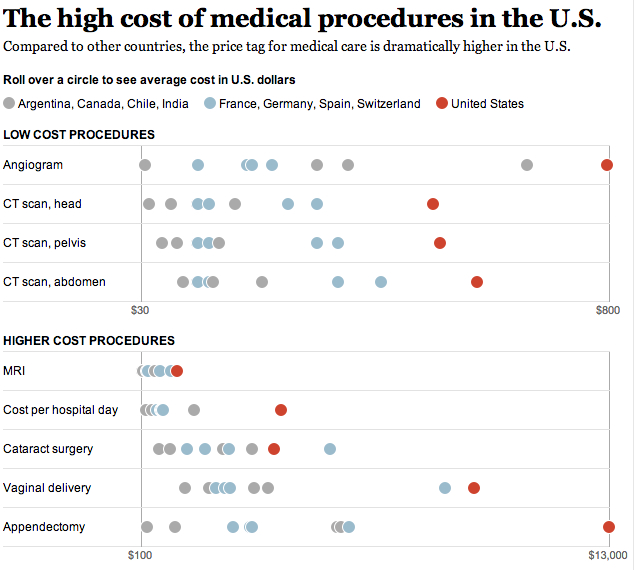
OK, so do the math. Near the top or at the top for utilization and over the top for prices = way over spending.
Of course, the last graph speaks to prices, which I’ll get to in the next post.
The Da Vinci Robot
My final target in this post is…Robotic Surgery. This is the penultimate waste of money, and the story is like something out of a movie.
The only robot being successfully marketed is the Da Vinci Robot. The Da Vinci robot is made and sold by Intuitive Surgical. Originally, there were a couple of companies developing surgical robots, but, Intuitive Surgical bought them out, leaving themselves as the only company making and selling them. Why wasn’t this considered anti-trust? A monopoly?
For those of you who don’t know what this thing is, here’s a picture of it. Notice the surgeon isn’t anywhere near you.

The robot costs about $2,000,000. For approximately 90% of the surgeries done using the robot, there is no clear benefit to doing the surgery with the robot. There may be some very special micro-type surgeries (like inside a chamber of the heart) where the robot is better, but, for the rest of the surgeries, there isn’t a benefit and sometimes, the non-robot surgery has a better outcome. I’m not going to quote all of the references for these statements, you can easily Google for this info yourself.
Here are some quotes from the literature about the Da Vinci Robot:
AHRQ:
Take-Home Points
- Robotic surgery is a rapidly expanding technology that has found a niche in multiple different surgical specialties worldwide.
- Although robotic-assisted surgery shows some short-term benefits surrounding the direct perioperative period, it has fairly equivalent long-term outcomes when compared to open surgery.
- Robotic surgery is generally safe with low overall complication rates, but adding the robot to the surgical equation inserts another potential entry point for error into an already complex and risk-fraught arena.
- In general, surgical outcomes are ultimately a direct manifestation of the skill and experience of the surgeon, not the technology or approach used.
They are basically saying you aren’t getting much for the cost of the robot and it adds complexity. FYI, Robot surgeries are longer than laparoscopic or open surgeries, and, ask any anesthesiologist or surgeon, the longer you are knocked out, the more likely you are to have a complication, including death.
The Lancet Study; 2016
“In the USA, 80-85% of prostatectomies are done robotically, and although the proportion is lower in the UK and Europe, it is increasing. Robotic surgery is more expensive than open surgery (the initial cost of the robot is approximately £1.5 million) and to date, there have been no randomised controlled trials comparing robotic with open surgery.”
“Surgery has long been the dominant approach for the treatment of localised prostate cancer, with many clinicians now recommending the robotic method to patients. Many clinicians claim the benefits of robotic technology lead to improved quality of life and oncological outcomes. Our randomised trial, the first of its kind, found no statistical difference in quality of life outcomes between the two groups at 12 weeks follow-up.”
I have a ton of articles stating similar to the above. To this date, there is no convincing evidence that the robot adds anything.
And then there are adverse events attributed to the robot itself that wouldn’t be in existence if it weren’t for the robot:
From: Adverse Events in Robotic Surgery: A Retrospective Study of 14 Years of FDA Data By Homa Alemzadeh1, et al, PLOS One, April 20, 2016
“During the study period, 144 deaths (1.4% of the 10,624 reports), 1,391 patient injuries (13.1%), and 8,061 device malfunctions (75.9%) were reported. The numbers of injury and death events per procedure have stayed relatively constant (mean = 83.4, 95% confidence interval (CI), 74.2–92.7 per 100,000 procedures) over the years.”
“Device and instrument malfunctions, such as falling of burnt/broken pieces of instruments into the patient (14.7%), electrical arcing of instruments (10.5%), unintended operation of instruments (8.6%), system errors (5%), and video/imaging problems (2.6%), constituted a major part of the reports. Device malfunctions impacted patients in terms of injuries or procedure interruptions. In 1,104 (10.4%) of all the events, the procedure was interrupted to restart the system (3.1%), to convert the procedure to non-robotic techniques (7.3%), or to reschedule it (2.5%).”
Here’s some cost and utilization stats:
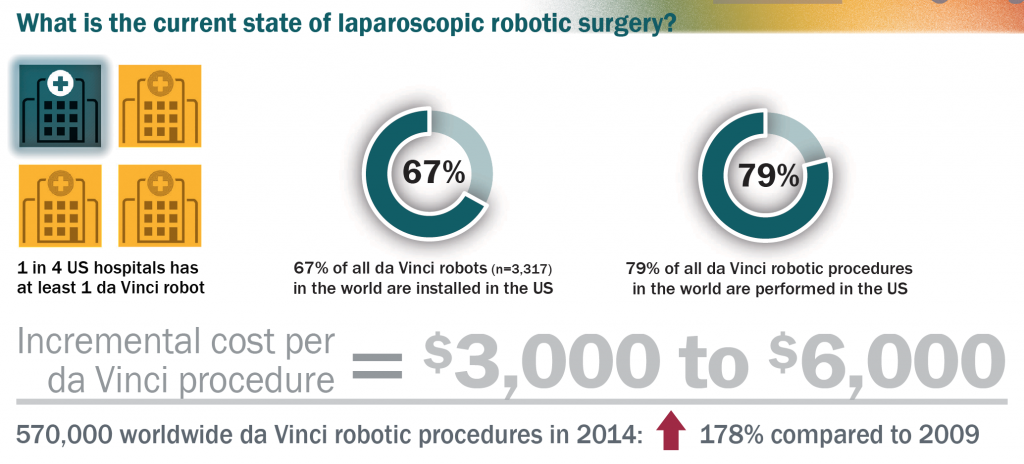
Notice the US has most of the robots and is doing most of the robotic surgery. There are several reasons for this.
- Intuitive Surgery is great at marketing and showing this bright shiny object to surgeons while having no good data to back up their marketing claims. It is amazing to see the faces of surgeons when the Da Vinci guys come to make their pitch. I’ve actually been at one of these. The surgeons act like kids in a candy shop. They are about ready to whip out their own credit cards to buy one. Then the Intuitive Surgery salespeople just have to step back and watch the surgeons tell the hospital administration that they will go to the hospital down the street, who has already bought a robot, to do their surgeries if this hospital doesn’t buy one. The administrators turn white thinking of how much surgery volume they could lose and immediately sign on the bottom line. This happens all the time, by the way, surgeons threatening hospitals to get things they want whether the things have been vetted in the literature or not.
- The current practicing surgeons grew up in the video game generation. And using the robot is just like playing a video game. Why do a surgery looking through a monocular laparoscopic tube when you can do one with a device that mimics playing a video game? Who knows, maybe pretty soon there will be global robot surgery competition like the video gamers are having now! Who can do the prostatectomy the fastest without a complication! I can see it now!
- This is the real crux of the robot issue. And the academic training centers in the USA are mostly to blame. They are supposed to be data-driven cultures who advocate doing things as proven in the peer reviewed literature. Well, in the case of the Da Vinci Robot, that couldn’t be farther from the truth. You see, most academic training centers have more than one Da Vinci robot. They are ignoring the peer reviewed literature. And the interns and residents use the robots pretty much exclusively. Which means, none of them are trained to do the laparoscopic or open procedures.
Here’s how this plays out.
As is usual in healthcare institutions, annually, there is a “budget crisis”. A couple of years ago, after a “budget crisis” call to find ways to reduce costs, I amassed a ton of data showing the robot didn’t add anything except adverse events and costs. I had a very compelling case. It was so good, the COO said he believed the robot wasn’t worth it BUT, a. the surgeons would defect if he shut it down and, b. he wouldn’t be able to recruit surgeons, especially Urologists and OB/GYNs because THEY COULD ONLY DO ROBOTIC SURGERY NOWADAYS. So, Intuitive Surgery has created it own self-fulfilling prophesy! This has to be the most arrogantly successful marketing strategy in the history of medicine! And the academic medical centers just went along with it!! Unbelievable!!
When you mention the extra costs (not human costs, just financial costs) for robotic surgery, some people say, “Well, it doesn’t matter because the hospital gets the same reimbursement whether they do a robotic or non-robotic surgery. It’s the same charge impact on the patient and insurance company.” What a naïve statement! Having watched how hospitals manipulate their charges and insurance company contracts, I can tell you that they aren’t simply going to take a $3000 hit on these surgeries. They figure out someplace else where they can increase reimbursement to, at the least, even it out and recoup that “loss”.
Addendum October 27, 2017: Two articles and an editorial in JAMA continue to confirm that the most Da Vinci Robots do is add to the cost of a surgery:
Association of Robotic-Assisted vs Laparoscopic Radical Nephrectomy With Perioperative Outcomes and Health Care Costs, 2003 to 2015; In Gab Jeong, MD, PhD; Yash S. Khandwala, BS; Jae Heon Kim, MD, PhD; Deok Hyun Han, MD, PhD; Shufeng Li, MS; YeWang, PhD; Steven L. Chang, MD; Benjamin I. Chung, MD; JAMA. 2017;318(16):1561-1568. doi:10.1001/jama.2017.14586
Effect of Robotic-Assisted vs Conventional Laparoscopic Surgery on Risk of Conversion to Open Laparotomy Among Patients Undergoing Resection for Rectal Cancer:The ROLARR Randomized Clinical Trial; David Jayne, MD; Alessio Pigazzi, PhD; Helen Marshall, MSc; Julie Croft, BSc; Neil Corrigan, MSc; Joanne Copeland, BSc; Phil Quirke, FMedSci; NickWest, PhD; Tero Rautio, PhD; Niels Thomassen, MD; Henry Tilney, MD; Mark Gudgeon, MS; Paolo Pietro Bianchi, MD; Richard Edlin, PhD; Claire Hulme, PhD; Julia Brown, MSc; JAMA. 2017;318(16):1569-1580. doi:10.1001/jama.2017.7219
Robotic-Assisted Surgery Balancing Evidence and Implementation; Jason D.Wright,MD; JAMA October 24/31, 2017 Volume 318, Number 16
Summary
- The USA utilizes high priced technology more than almost all other nations.
- Technology is preferred over actually seeing and examining patients by today’s practitioners.
- High Priced Technology utilization is “overtreatment” and is one of the two most prominent drivers of USA health care costs.
- The EMR exacerbates the technology reliance by today’s practitioners.
- The Da Vinci Robot adds cost and adverse events without evidence that the patient benefits from it.
- Intuitive Surgery has a “death grip” marketing strategy, adopted by academic medical centers, that guarantees it’s continued sales of a device that shouldn’t be used.
- It would take the medical community, led by the academic medical centers, being willing to “bite the bullet” and say “no more of this” to Intuitive Surgery and shut down the robots and train surgeons in the non-robotic surgeries to phase out the robots. But, since it’s all about the money, that is probably an unlikely scenario. And the medical community is relatively gutless anyway. Witness the Opioid epidemic…which never should have gotten to the point it did and wouldn’t have if the medical community stood up to The Joint Commission and the drug companies.