Why The US Healthcare Care System Costs So Much – Part Two – Care Coordination
The second waste category in Berwick and Hackbarth’s JAMA article is “Failures of Care Coordination”. Berwick and Hackbarth define this as “the waste that comes when patients fall through the slats in fragmented care.” Berwick and Hackbarth state further, “The results are complications, hospital readmissions, declines in functional status, and increased dependency, especially for the chronically ill, for whom care coordination is essential for health and function. We estimate that this category represented between $25 billion and $45 billion in wasteful spending in 2011.”
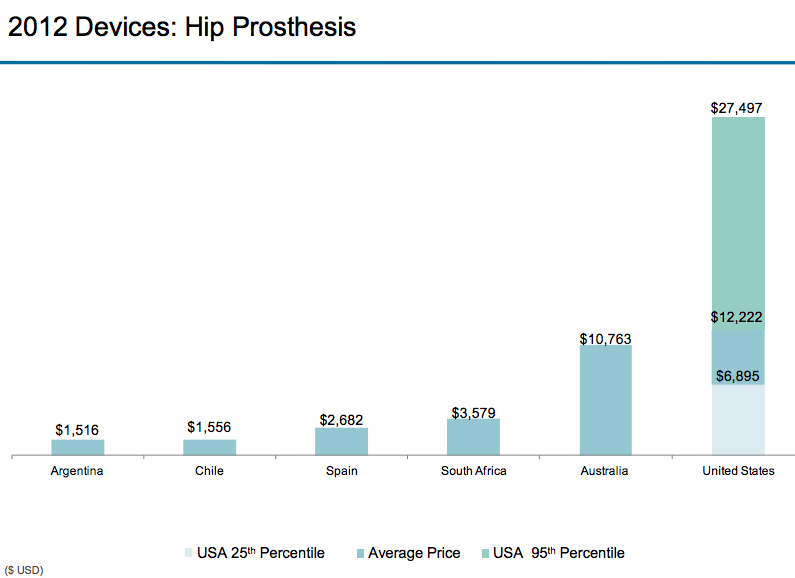
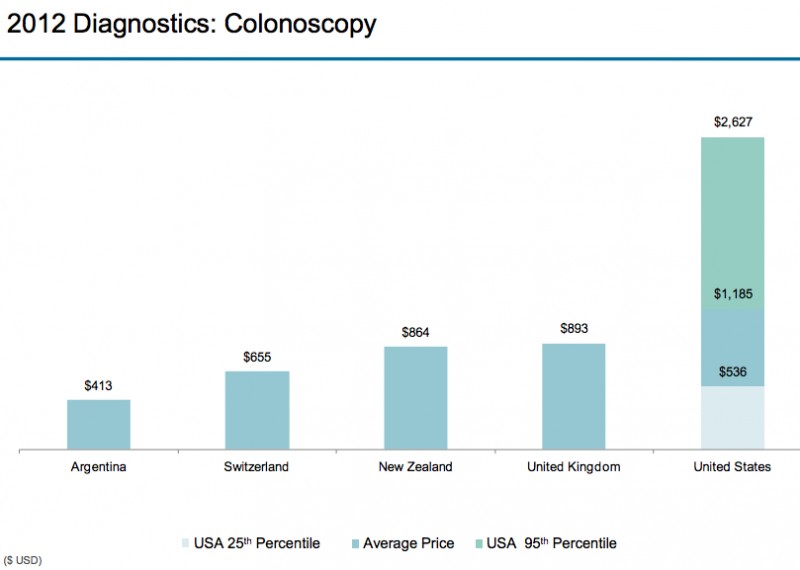
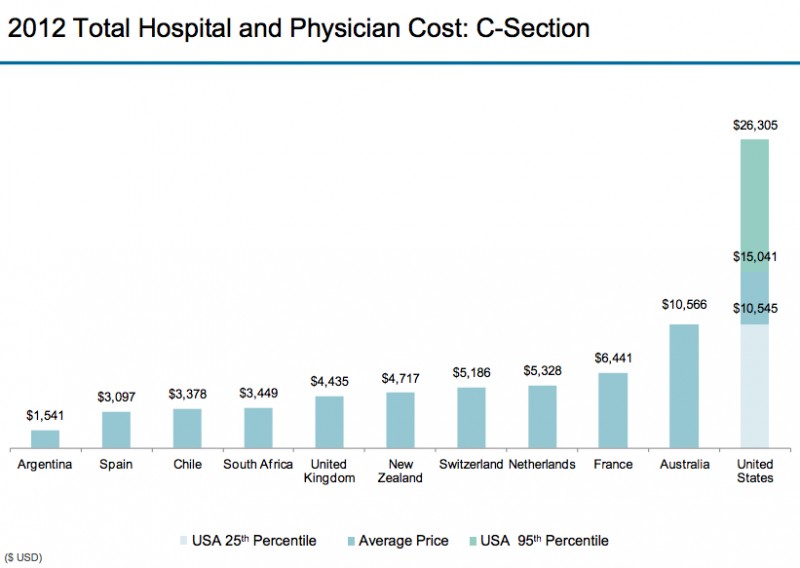
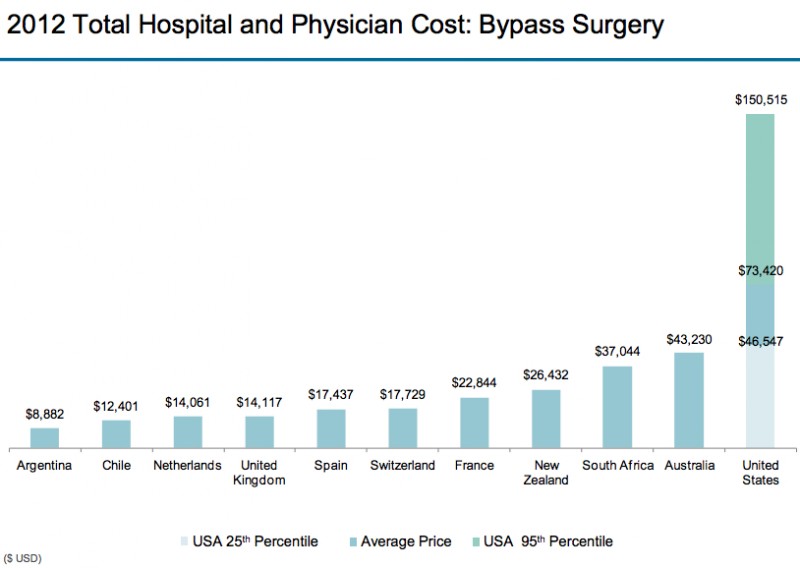
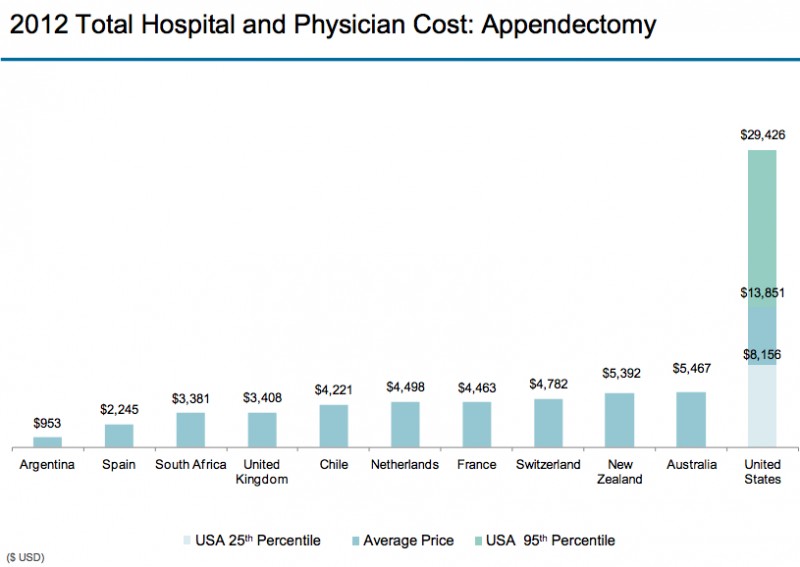
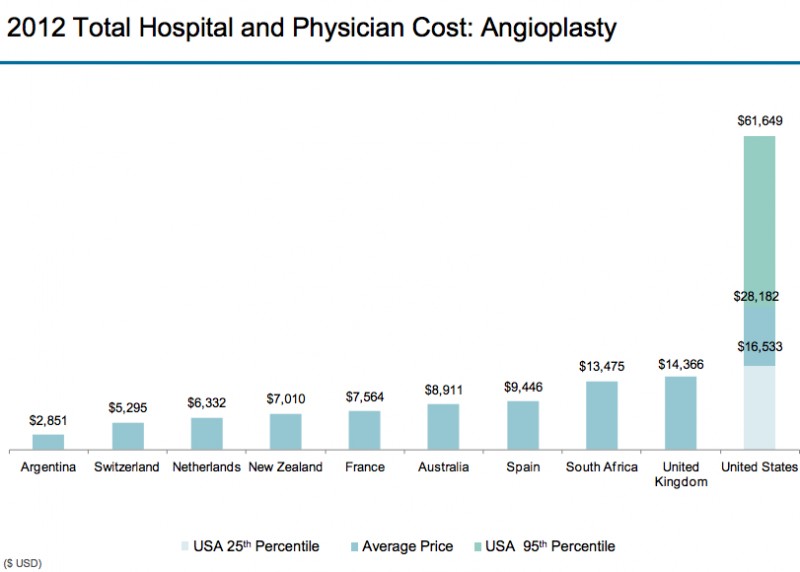
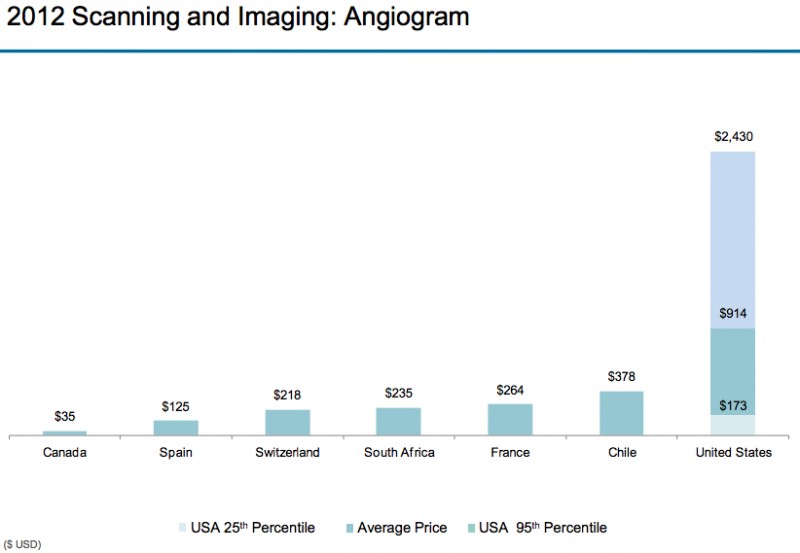
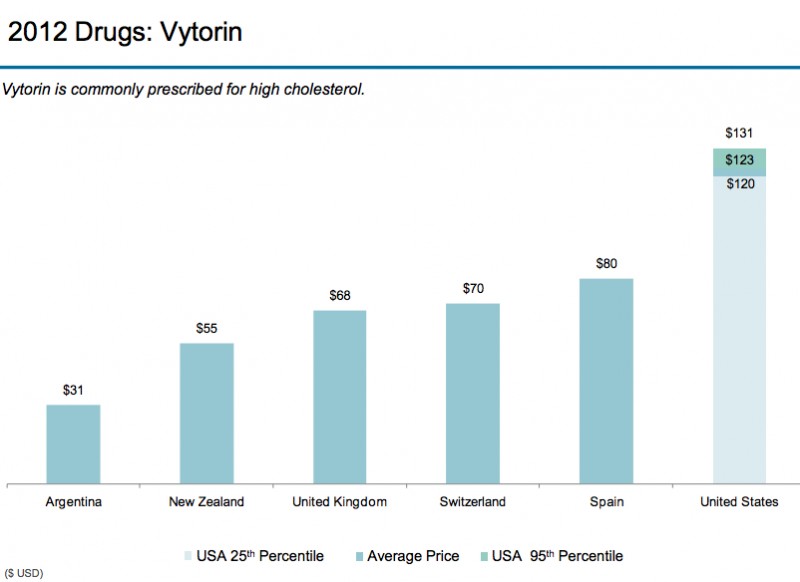
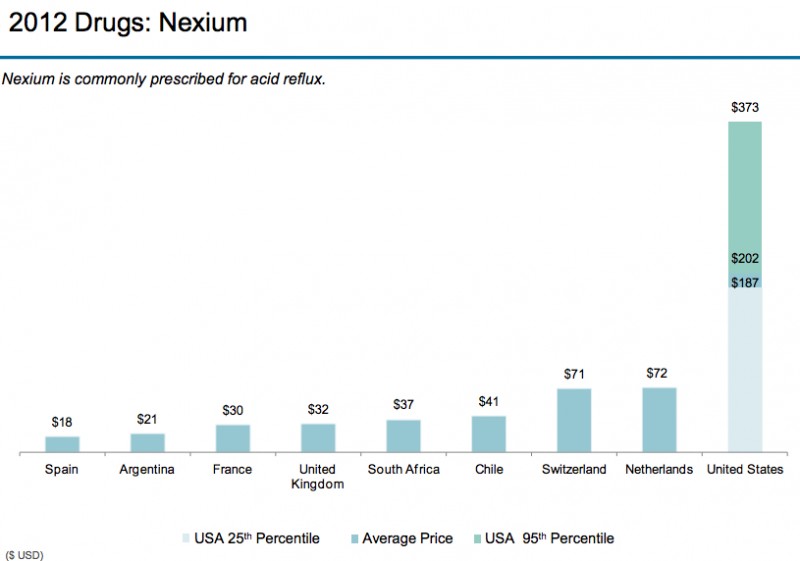
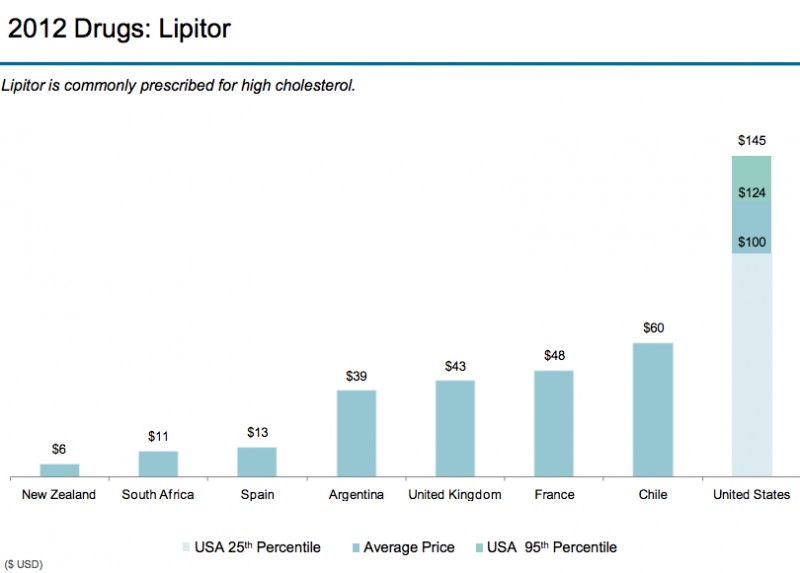
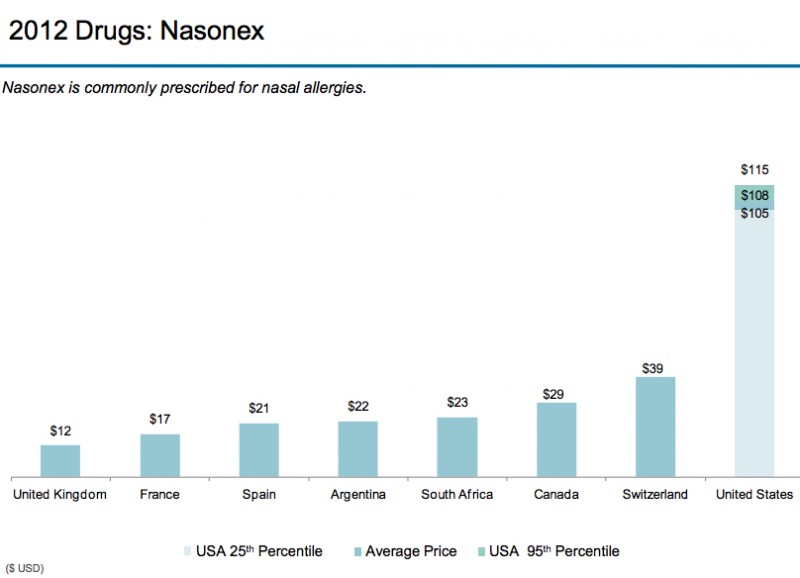
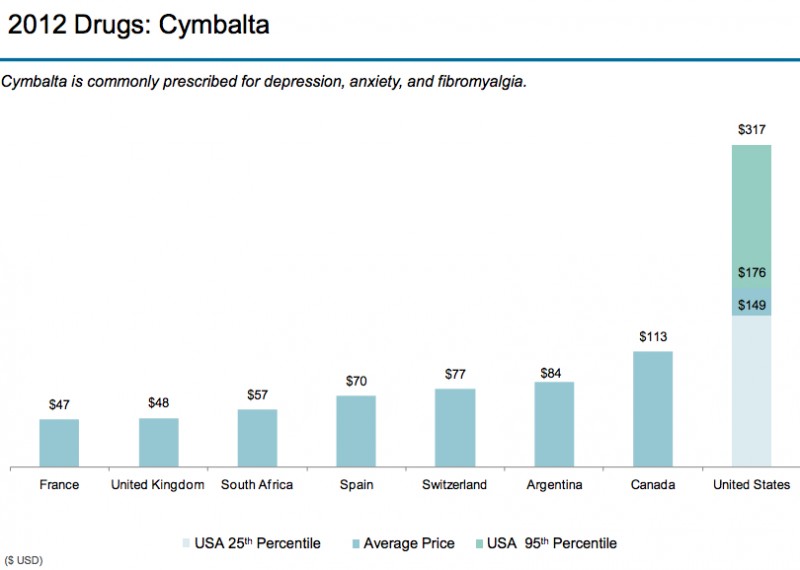
$25 billion and $45 billion sounds like a big number, but, compare that to between $102 billion and $154 billion for Care Delivery Failures, $158 billion and $226 billion for Overtreatment, $107 billion and $389 billion for Administrative Complexity, and $84 billion and $178 billion for Pricing Failures. Obviously, it is much less. Note that Berwick and Hackbarth don’t mention the cost offset in administrative costs to “care coordinate”. Their estimated savings can easily be wiped out with the added administrative costs to “care coordinate.”
Now, if you haven’t read my post on the fragmentation of the US health care system, you should do that before reading this post any further. It’s under the “General” category called “The Fractured US Health Care System”.
The bottom line for fragmented care is, the priorities of practitioners (MD’s, DO’s, APC’s) have caused the largest component of fracturing/fragmenting. There have always been “silos” in health care (referring to monolithic structures inherent in the health care system: Physicians, Hospitals, Ancillary services, Pharma, Device Manufacturers, etc.) since its inception but the true fracturing of the system is the result of practitioners. This fracturing has led to a huge hand-off and communications gap. Like, Grand Canyon huge. Care Coordinators/Case managers are supposed to bridge these gaps.
Here’s one of many examples of the hand-off/communication gap.
PCP’s often don’t know their patients are admitted to a hospital. Unless the PCP sends the patient from his/her office, they don’t know the patient was sick enough to be admitted. This is because the PCP either sends the patients to the ER or Urgent care when they call with a problem or the patient just shows up there. Then, they get admitted. The hospital has Hospitalists so they don’t need to call the PCP. Remember that PCP’s don’t go to the hospital so they aren’t on the hospital medical staff. If a physician is not on the medical staff they have no access to the hospital electronic medical record (EMR or its notification system).
If a hospital system has a medical group, they can message the PCP in their medical group that the patient is in the hospital using internal messaging systems or through a unified EMR. If the PCP is not “owned” by the hospital, they are, 99% of the time, either on a different electronic medical record or still using paper. Some EMR’s that the hospitals use have the ability to connect the non-owned PCP with a “Physician Portal” which is usually a read-only version of the medical record; however, unless a PCP signs on and looks to see if any of their patients are admitted, they don’t know about it. The PCPs we talked to wanted hospital information integrated into their own EMR as they felt it was too much extra time to be signing on to a hospital physician portal (which timed out frequently).
I was leading a readmission reduction effort at a hospital system. They had a large Medical Group and the hospital system tended to focus on their Medical Group to the exclusion of the non-Medical Group PCPs. Our analysis showed that 50% of the hospitals’ discharges were to non-Medical Group PCPs. We ranked the non-hospital owned PCP practices by percent readmissions and targeted the top 20 practices. We then visited the practices, showed them their data to the patient level and asked them if they had any ideas as to why their practice had such a high readmission rate. Some of the patients had four readmissions in a 3-4 month time period.
The PCP’s unanimously said they didn’t know the patients were even admitted to the hospital, they didn’t get a notification from the hospital that the patient was discharged, and they had no idea whether the patient went home or to a skilled nursing facility or nursing home. One doctor said (exact words), “ I only know what happens to these patients if they eventually make it to an appointment with me or I read their obituary in the newspaper.” In addition, most of the practices said, “You know, if we knew when our patients were discharged, we could have one of our nurses contact them and make sure everything is going OK and give us a status update so we could make sure we see the patient in a timely fashion. It’s part of our nurse’s job.” These PCP offices had “transition of care” nurses! Who knew the patients! And weren’t being utilized! How wasteful is that?
The other thing that is problematic is, when the patient gets admitted to the hospital, there is no verbal hand-off between the PCP and the Hospitalist. And when the patient is discharged, there is no verbal hand-off between the Hospitalist and the PCP. The Hospitalists actually say they won’t call a PCP, and since the PCP doesn’t know the patient is admitted, the verbal hand-off at the time of admission can’t happen. When we “old docs” were doing both office and hospital work, this wasn’t a problem. And, back then, if another physician admitted the patient (e.g., the patient was admitted from the ER with appendicitis to a surgeon’s service) the ward clerk always called your office to notify you that the patient was admitted. Repeat… CALLED YOU! Now everyone wants an IT solution. It’s like millenials want to text instead of talk with a smart phone.
So, nationally, because of Medicare and the Readmission Reduction program, which has penalties for higher than expected readmission rates, hospitals and health plans are hiring nurses and ancillary staff to “care coordinate” discharges from the hospital. Isn’t this more expensive than a phone call and accessing resources already present in the PCP office? Duplication of resources is a process waste category.
OK, now that you have seen but one out of the hundreds of hand-off gaps, back to Care Coordination.
Before we really get into this subject, we need some definitions, because people throw around the words “case management”, “care coordination”, etc. with ambiguity and impunity. So, let’s look at definitions supported by some degree of credibility:
Integrated Care Management: The management and delivery of health services so that patients receive a continuum of preventive, behavioral health, curative and long term care services according to their needs over time and across different levels of the health system. (WHO; modified) This requires a combination of Case Management and Care Coordination.
Case management: A collaborative process of assessment, planning, facilitation, care coordination, evaluation, and advocacy for options and services to meet an individual’s and family’s comprehensive health needs through communication and available resources to promote quality, cost-effective outcomes. (Case Management Society of America) This requires a level of health care licensure, like, a Registered Nurse or “higher”. Case management has been around since about 1900, and historically was applied to a small number of patients with serious illnesses and complex care needs.
Care Coordination: Care coordination is the deliberate organization of patient care activities between two or more participants (including the patient) involved in a patient’s care to facilitate the appropriate delivery of health care services. (Closing the Quality Gap: A Critical Analysis of Quality Improvement Strategies (Vol. 7: Care Coordination)). Unlicensed staff can do this. It is essentially project management. Licensed professionals design a series of steps or activities and a care coordinator tries to make sure they all happen. Care coordinators don’t necessarily give medical advice or apply medical judgment. At the same time an RN or practitioner can be a care coordinator; it’s part of their job description.
Care Management: A set of individualized, goal-oriented, culturally relevant and logical steps to assure that a patient receives needed services in a Safe, Timely, Effective, Efficient, Equitable, Patient-Centered and cost-effective way. (Accenture; modified) This is like a “project plan”, which someone acting as a care coordinator can facilitate.
“Care Coordination” nowadays is a health care industry “fad” that dominates the thinking of health care systems and has spawned numerous vendors selling care coordination services and supporting IT systems. It is extremely reminiscent of the Disease Management programs that dominated the health care industry in the mid 1990’s and first ten years of the 21st century.
Interestingly, there are no significant Disease Management (DM) companies peddling their services or supporting IT systems anymore. Why? They couldn’t reliably show cost savings. Remember, it’s all about the money. If a health care program can’t show some dollars falling to the bottom line, it will eventually be discontinued. If you want to know why Disease Management couldn’t show sustainable results, read Why Nobody Believes the Numbers by Al Lewis. The same thing is happening with Care Coordination. DM companies would come to your offices and show examples where they said they got large health care cost savings. Millions and millions of dollars. So health plans would hire them, run the program and find little or no cost savings. This is because the DM programs measured incorrectly. That’s what Al Lewis’ book is all about.
Well, the same thing is happening with Care Coordination results. If you see an article or a vendor offering Care Coordination and they are saying the results are eye-popping, like $84 million savings in two years, you can pretty much bet they aren’t measuring it correctly, because, as you will see below, the real hard data doesn’t support this contention.
So, I’m here to tell you that Care Coordination is very similar to the now defunct Disease Management companies. Care Coordination and Case Management (combined called Care Management) programs are major pillars in Population Health programs, are touted as the saviors of the cost and utilization problems of the health care system. Health systems and Health Insurance Plans have hired thousands of, usually, RN’s out of the face-to-face patient care venues to sit at computers and, mostly, telephonically “care coordinate” selected patients (or members/beneficiaries if it’s a health plan).
Problem #1: This mass hiring of nurses has exacerbated the nursing shortage in hospitals and outpatient caregiver arenas.
Problem #2: The cost savings are paltry compared to other interventions to reduce costs. And the activity adds dollars to the administrative costs, which are already too high.
Problem #3: Case management and care coordination have shown very limited impact on utilization and quality improvements.
But don’t take my word for it. The Agency for Healthcare Research and Quality (AHRQ) is a federally funded, industry unbiased agency whose role is “to produce evidence to make health care safer, higher quality, more accessible, equitable, and affordable, and to work within the U.S. Department of Health and Human Services and with other partners to make sure that the evidence is understood and used.”
The AHRQ released a 542-page analysis of 153 articles representing 109 studies of case management/care coordination programs. Here’s their conclusion:
“Recognizing the heterogeneity of study populations, interventions, and outcomes, we sought to elucidate the conditions under which CM was effective. We found that CM had limited impact on patient-centered outcomes, quality of care, and resource utilization among patients with chronic medical illness.”
Not convinced?
Read “Cost Containment and the Tale of Care Coordination” by J. Michael McWilliams, M.D., Ph.D. in New England Journal of Medicine 375;23 December 8, 2016. Here’s his two cents:
“Though attractive, this notion is not evidence-based. Studies of programs or practice models designed to enhance coordination and management of care for patients with multiple conditions and multiple providers have shown minimal, if any, consistent savings.
There are several reasons for this lack of savings. First, efforts to coordinate care and improve patient outcomes appropriately involve interventions to correct underuse and ensure timely access to care. In isolation, these efforts tend to increase the use of care, at least partially negating any reductions in preventable or unnecessary care resulting from coordination. Second, the “number needed to treat” is greater than one. And third, coordinating care is costly.”
So, according to these two experts (who have plenty of supporting evidence), the health care world is spending a lot of money to get, well, not much. All the other waste categories have, like 10 times the savings opportunity!
Here’s a graph from the Berwick and Hackbarth article showing this. Notice how thin the Care Coordination stripe is.
I suspect you would get more bang for the buck if you re-deployed these nurses to do more face-to-face caring for patients integrated with PCP and Specialty practices. This is just my suspicion. No one’s doing it so I don’t know of any credible data.
And then there is the persistent focus on care coordinating high cost cases. This is a sacred cow promoted by the health care finance departments that should be slaughtered and made into steaks and hamburgers. Yes, the CFO’s of the health care industry are telling health care professionals what to do. They have been so forceful, persistent and vociferous that the rest of the industry has been totally brainwashed into thinking, as in the words of gangster Willie Sutton, “that’s where the money is.” [Just an FYI, the finance departments, supported by the MBA-type health care industry administrators, are the real authoritarians in health care institutions. What they want, they generally get. They ignore the medical professionals telling them they are wrong. They don’t really care about anything but the bottom line being black. No, that’s not right. They want to meet their profit margin projections. I’ll be doing a post totally dedicated to this phenomenon. They generally view the medical professionals as a necessary evil they have to manage.].
Here’s why this high cost case management myth exits.
As claims (A claim is a bill sent by a health care provider to an insurance company. When it enters an insurance company it is re-named a claim.) come into the insurance company, it gets “credited” to the beneficiary. When the dollar amount of the claims reaches a pre-determined amount, it is placed on a high cost case list. Usually, the amount is between $50,000-75,000. This list is generated often, usually weekly if not daily. The finance department wants this list “worked” and wants the Medical Management staff to do something to limit any further claims coming in. They think there is definitely something that can “stop the hemorrhage” of dollars. You can’t imagine the panic, shock and anger the finance people display if you can’t, as medical professionals, stop the claims from coming in. And, the finance people have absolutely no understanding of what clinical courses the patients are going through nor do they have any evidence that something material can be done about the costs of these cases. They just want what they want….fewer claims. They want you to deny care, for example. A denial means no cash out. Instant savings.
The high cost cases are usually catastrophic cases. Major trauma. Neonates (premature births) with major complications. Conditions like sepsis, cardiogenic shock, respiratory failure, which include multiple organ failures. These people are in ICU’s and are usually not in any condition to be transported. Their costs can run up to a million dollars. Finance folks literally freak out over these cases.
You’ll hear and read statistics like 10% of the populations spends 50% of the health care costs. Yes, that’s true. But, I’ll show you why that statistic can’t be changed much. Because THERE WILL ALWAYS BE A TOP 10%!!! Just because the top 10% cost cases spend 50% of the health care dollars doesn’t automatically translate that you can save anything by focusing on these cases.
It turns out, there is little you can do for these folks. They are incredibly sick. Your best option is to broker a better case rate with the hospital and deploy a case manager to urge (not make) the medical staff to move the patient along the care course as quickly as the patient’s condition will permit and create an excellent discharge plan.
In the early 1990’s a really smart physician named Richard L. Doyle, MD analyzed hospital data and noticed significant variation in hospital utilization rates for the same conditions among several hospitals where he was working. He developed guidelines for inpatient conditions that supported the treatment of patients according to their physiologic status. These were originally called Milliman and Robertson Care Guidelines and are now called MCG guidelines. You can Google this. One thing Dr. Doyle stressed was, don’t spend a lot of time on the exceptionally sick patients. Do what you can to facilitate their care, but, you won’t see significant cost savings from that activity. What he stressed was making the care of the routine, high volume cases as efficient and appropriate as possible; that’s where the money is. Shave a few hundred dollars off of hundreds of cases and you saved hundreds of thousands of dollars.
I’ve actually done analyses on populations of people and shown this to finance people, but they never listened. The savings basically look like a bell curve with the seriousness of the illnesses on the X-axis and the savings on the Y-axis. The low-serious cases have low savings because these people aren’t very sick, spend little money and get better quickly. The upper end of the curve is low savings because they are relatively small numbers (remember only 10% of the population) and there isn’t much you can do to affect their clinical course. It’s the middle 40% or so where the volume is high and you can actually alter their clinical course by mitigating overtreatment and reversing under-treatment where you get savings. I actually have real data in bubble graphs that prove this. It supports Dr. Doyle’s contention. No finance person would acknowledge this data. I was in one health plan where the VP of Medical Affairs wanted to stop working the high cost case list because the administrative cost for working the list was at or slightly more than the savings. Alas, the Finance folks got their way and she was ordered to keep working the list. Stopping was heresy.
The other thing I saw in the data was, most of the people in the top 10% cost strata one year were not in that strata in the next year AND THERE IS STILL A TOP 10% SPENDING 50% OF THE HEALTH CARE COSTS!! Here are the reasons: 1. The person died, 2. The person had a self-limited catastrophic event (a health attack, a car accident, a severely premature infant who is now home, etc.), 3. There is a residual (minority) of really sick people who are still in the top 10% and spending money because they need the care (like cancer patients). The next year has 10% spending 50% because there are new cases of self-limited catastrophic events or people so sick that they are dying. The real trick is to work on that 40% to limit the catastrophic cases with pre-emptive activities instead of “beating a dead horse” who has already left the barn.
You have no idea how many times and in how many companies I showed the finance people this information. But they were still persistent and vocal and perennially complained to the “Administration” about the lack of effectiveness of the Medical Management departments in reducing the cost of top 10% cases through “managing” them. They still don’t understand that this is like playing “Whack-a Mole”.
But, again, don’t just take my work for it.
Read an article titled For Many Patients Who Use Large Amounts Of Health Care Services, The Need Is Intense Yet Temporary by Tracy L. Johnson, et al from Health Affairs, August 2015. Here is their finding:
“Our analysis found that consistently 3 percent of adult patients met super-utilizer criteria and accounted for 30 percent of adult charges. Fewer than half of super-utilizers identified as such on May 1, 2011, remained in the category seven months later, and only 28 percent remained at the end of a year.”
Here’s the graph about this. It is similar to what I had seen for years. Notice the really small red section at the bottom of the bars. Those are the ones who are year over year in the top 10%. Most of the rest of them disappear from the list.
Here’s another validating article: “Focusing on High-Cost Patients — The Key to Addressing High Costs? by J. Michael McWilliams, M.D., Ph.D., and Aaron L. Schwartz, Ph.D., New England Journal of Medicine, March 2, 2017.
“Targeting patients with high spending may not effectively target the spending that should be reduced. Longitudinal patient specific investments that are important for coordinating care and improving quality may be less important for curbing wasteful spending.
Thus, a focus on high-cost patients may not only fail to contain health care spending, it may help to entrench the status quo, since targeting specific patients suits existing provider structures developed under fee-for-service incentives”
Here’s a third article validating my assertions about high cost cases. I actually had a consultant tell me I didn’t know what I was talking about, that I didn’t “get it”. He specifically emphasized managing End of Life Care patients in the top 10%. Google this article and read it, it’s an exhaustive data-based study saying virtually the same thing as above. The article is: The Myth Regarding the High Cost of End-of-Life Care by Melissa D. Aldridge, PhD, MBA, and Amy S. Kelley, MD, MSHS, American Journal of Public Health, December 2015, Vol 105, No. 12, p. 2411.
Again, with high cost cases you do what you can to get the best price and urge or assist the caregivers to be efficient, but the cost savings are minimal for high cost cases. And this finance proposed activity just increases administrative costs.
Maybe soon, health care administrators and finance folks will realize that care coordination and the high cost case focus aren’t the cost savers they think they are, will reduce the number of care coordinators and case managers, let the nurses get back to directly caring for patients (maybe in ways that are not traditional), focus on that middle 40% of chronically ill patients who need their care optimized at the primary care/specialty care level, re-design wasteful care process structures and work on optimizing the other five waste categories.
Right now, that’s a hard sell.
Now, there are some benefits to care coordination. They are its direct impact on the patient. It may improve their quality of life. It may simplify their condition management regimen. It might reduce a patient’s out of pocket costs. It might improve their feeling of well-being. But it doesn’t significantly bend the medical cost curve, if it bends it at all.
And, as you will see, improving four of the other five waste categories actually improves the health status of the “middle 40%” cost patients. (Fraud and Abuse being the outlier)
Summary:
Care coordination does little to improve patient outcomes, quality measures, utilization and costs.
Current Care Coordination activities divert the nurse and practitioner work force from direct caring of patients to working on an activity with limited impact, exacerbating nurse and practitioner shortages.
Focusing on high cost cases does not save a lot of money and distracts caregivers from optimizing the care of patients with chronic illnesses and poor health status.
Care coordination may have a positive impact on individual patients felling of well-being. There is no good data I know of that proves this.

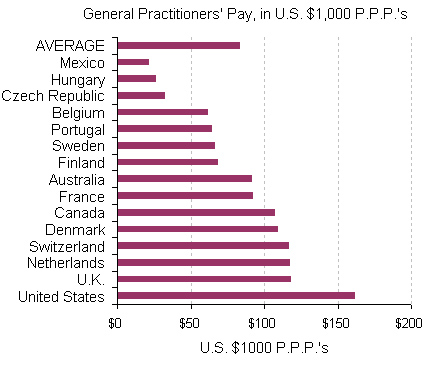

 (Source: Modern Healthcare August 3, 2017)
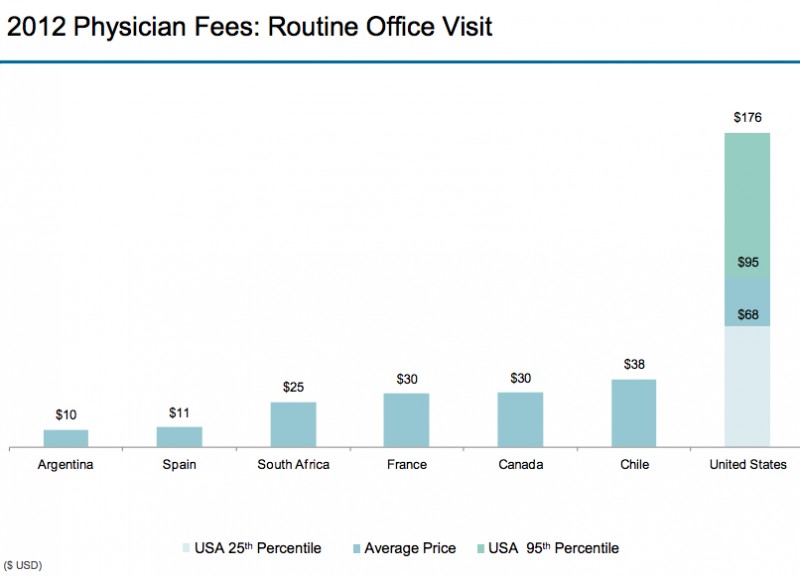
(Source: Modern Healthcare August 3, 2017)